Figures & data
Table 1 Demographics for Study I (open-label 4-week study consuming 1 g ACE daily)
Figure 1 Study design for the open-label pilot study on the aqueous cyanophyta extract (ACE) from Arthrospira platensis.
Notes: One gram of ACE was consumed daily for 4 weeks. At baseline, each person’s primary and secondary anatomical areas of chronic pain complaint were noted. Pain scores for these areas were collected at each subsequent visit, where each data collection visit is indicated by an arrow.
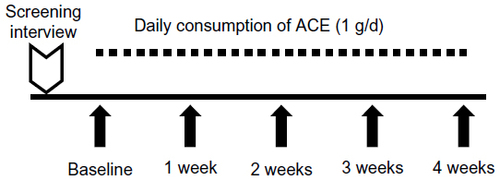
Table 2 Demographics for Study II (placebo-controlled crossover dose study)Table Footnotea
Figure 2 Study design for the single-blind, placebo-controlled dose study.
Notes: Placebo (0 mg product) as well as 250 mg and 500 mg aqueous cyanophyta extract (ACE) were each consumed for 7 days, by all study participants, separated by a 7-day washout period. The order in which each study participant consumed placebo versus 250 mg and 500 mg ACE is as indicated on the diagram; however, the test products were of similar appearance and were blinded and unknown to the study participants. At baseline, each person’s primary and secondary anatomical areas of chronic pain complaint were noted. Pain scores for these areas were collected at each subsequent visit, where each data collection visit is indicated by an arrow.
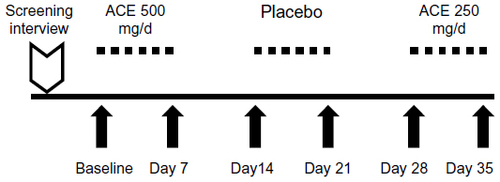
Figure 3 Data on pain scores collected by visual analog scales (VAS) during Study I.
Notes: Data are shown for the primary (top) and secondary (bottom) pain complaint areas when at rest (solid lines) and when physically active (dashed lines). The average ± the standard error of the mean for the 12 study participants is shown for baseline and the four following weekly visits. Levels of significance of data sets when compared to baseline data are indicated by asterisks: a trend of P<0.1 is indicated by (*), significance P<0.05 indicated by *, high statistical significance P<0.01 indicated by **, and a very high level of statistical significance P<0.001 indicated by ***.
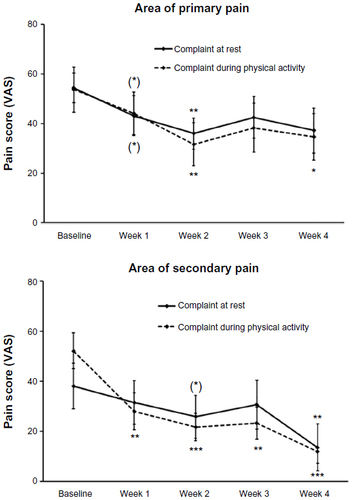
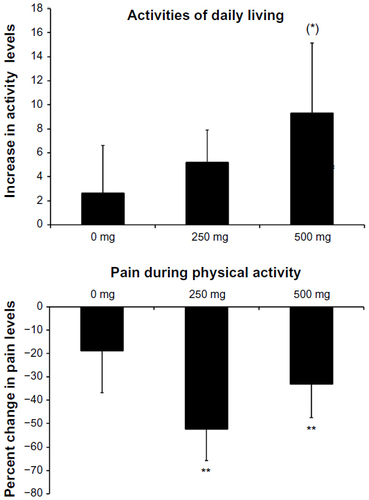
Figure 4 Data on activities of daily living questionnaire and pain level during physical activity were collected during Study II.
Notes: Data on activities of daily living (top) are shown as the average ± the standard error of the mean for the changes recorded from baseline to the following visits, where either placebo (0 mg) or ACE at 250 mg or 500 mg was consumed daily. Data on pain scores (bottom) are shown for those people with pain scores at baseline over 5/100, thus excluding people with no pain during physical activities at the start of each 1-week study interval. After 7 days of consuming 500 mg ACE/d, participants were increasingly active. At both ACE doses of 500 mg/d and 250 mg/d, pain levels during physical activity were reduced. The combined data suggest that pain reduction allowed for an increased level of physical activity. Levels of significance of data sets when compared to baseline data are indicated by asterisks: a trend of P<0.1 is indicated by (*) and a high level of statistical significance P<0.01 indicated by **.
Abbreviation: ACE, aqueous cyanophyta extract.
Abbreviation: ACE, aqueous cyanophyta extract.