Figures & data
Table 1 Demographics, radiographs, intraoperative findings, and postoperative outcomes of the 25 patients with chronic and subacute subdural hematoma treated by neuroendoscopy
Figure 1 The basic steps of neuroendoscopic hematoma evacuation for chronic and subacute subdural hematoma.
Notes: (A) The patient was placed in the lateral position, and a straight scalp incision was made on the parietal region. (B) After a bone flap was created, the dura was suspended. (C) After the dura was opened in a cruciform fashion, the outer membrane of the hematoma was revealed. (D) The liquefied blood was slowly aspirated with a syringe to decrease the intracerebral pressure. (E) The residual hematoma and blood clots were evacuated by suction under the neuroendoscope. (F) Fibrin septa were checked and treated under the neuroendoscope. (G) A bridging vein was seen, and a draining catheter was introduced in the cavity under the neuroendoscope. (H) The bone flap was replaced and fixed.
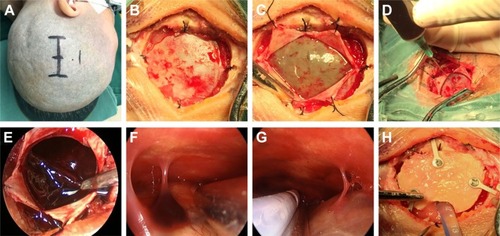
Figure 2 Neuroendoscopic surgery for subacute subdural hematoma.
Notes: (A–C) Preoperation CT scan showing a subacute subdural hematoma on the left side. (D–I) Hematoma evacuation under the neuroendoscope during the operation. (J–L) Post-operation CT scan showing the subtotal evacuation of the hematoma, regression of the midline shift, and ideal placement of the draining catheter.
Abbreviation: CT, computed tomography.
Abbreviation: CT, computed tomography.
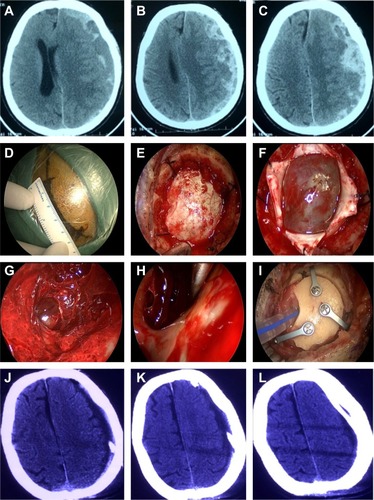
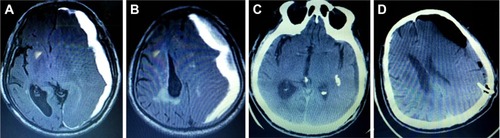
Figure 3 Neuroendoscopic surgery for recurrent CSDH.
Notes: (A) CT scan showing a CSDH on the right side. (B) MRI showing fibrin septa in the hematoma cavity. (C) CT scan showing the incomplete evacuation of the hematoma one day after the first burr-hole surgery. (D) CT scan showing hematoma reaccumulation 10 days after the first burr-hole surgery. (E) CT scan showing the hematoma in the subdural area 1 day after the second burr-hole surgery. (F) MRI showing that the hematoma had not disappeared 15 days after the second burr-hole surgery. (G) Operation view showing fibrin septa in the hematoma cavity during the third surgery via the neuroendoscope. (H) Forty days after the third surgery by neuroendoscope shows no recurrence.
Abbreviations: CSDH, chronic subdural hematoma; CT, computed tomography; MRI, magnetic resonance imaging.
Abbreviations: CSDH, chronic subdural hematoma; CT, computed tomography; MRI, magnetic resonance imaging.
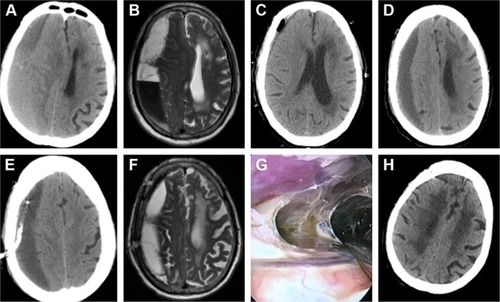
Figure 4 Incorrect placement of the draining catheter by burr hole.
Notes: (A, B) MRI showing a CSDH on the left side before the operation. (C, D) CT scan showing inadvertent placement of the catheter in the brain parenchyma after burr-hole surgery.
Abbreviations: CSDH, chronic subdural hematoma; CT, computed tomography; MRI, magnetic resonance imaging.
Abbreviations: CSDH, chronic subdural hematoma; CT, computed tomography; MRI, magnetic resonance imaging.