Figures & data
Table 1 Primary and supportive diagnostic criteria for FN
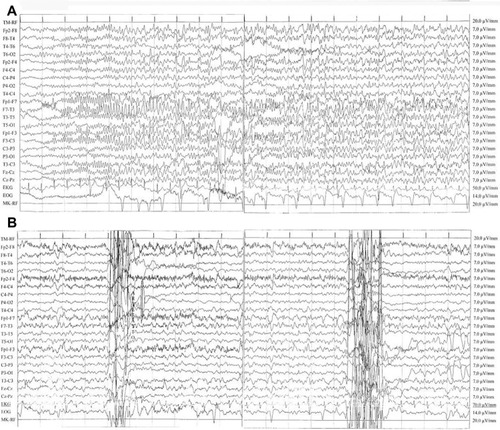
Figure 1 (A) Seizure with a left frontotemporal focus. Ictal electroencephalography (EEG) showed rhythmic and reluctant fast (12–13 Hz) activity primarily involving the left frontotemporal area consisting of polyspikes of about 100 mV amplitude with reversal phase in the F7 lead, then epileptic discharge involved all channels and showed a reduction in frequency (6 Hz). The patient was unconscious. Discharges consisting of high-amplitude sharp waves (90–100 μV) and slow waves (prominent on the frontotemporal areas) (high 30 Hz, low 0.1 second; rate 15 mm/second). (B) EEG during pseudoseizures. Normal background activity with interictal abnormalities in left frontocentrotemporal channels: sporadic and nonperiodic sharp waves at 100 mV with reversal phase on F7 and sporadic anterior synchronous and asynchronous theta activity (6–7 Hz, 50–60 mV). Muscular artifacts on right frontal derivations and two abrupt movement artifacts were concomitant with fictitious spasms of the patient. No epileptic seizures were recorded. This recording showed a significant reduction of interictal activity in comparison with her previous EEGs.