Figures & data
Table 1 Clinical Characteristics That May Assist with Distinguishing Testicular Torsion from Torsion of the Testicular Appendix and Epididymo-Orchitis
Figure 1 “Whirlpool sign” of the spermatic cord. (A) Gray-scale transverse US image of upper left scrotal sac shows an eddy swirl (arrow) of the spermatic cord suggesting torsion of the cord. This 12-year-old boy woke with acute left testicular pain and experienced nausea and vomiting along with the pain. (B) Power Doppler US image of the same twisted cord shows concentric pattern of preserved flow in the vessels of the twisted cord. The flow in the left testis (not shown) was minimally decreased compared to the right side and bilateral bell clapper deformity was found during orchiopexy along with complete torsion of the left testis with 360° twist. (C) Gray-scale longitudinal US image of the left scrotum in a 13-year-old boy with 1 day of left-side pain shows abrupt spiral twisting of the spermatic cord (arrow) at the external inguinal ring, creating a whirlpool sign. (D) Color Doppler transverse image of the testes in the same boy as in (C) shows preserved and symmetrical flow bilaterally. After manual detorsion in the emergency room, he underwent orchiopexy and was diagnosed with intermittent torsion. (Image obtained from Bandarkar AN, Blask AR. Testicular torsion with preserved flow: key sonographic features and value-added approach to diagnosis. Pediatr Radiol. 2018;48(5):735–744. doi:10.1007/s00247-018-4093-0.Citation27 Distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/). No changes have been made to the images or the image description).
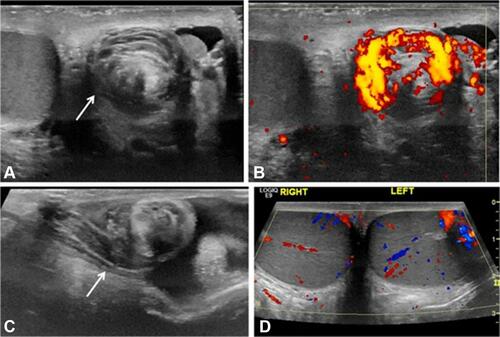
Figure 2 Intermittent torsion in a 17-year-old boy who presented with 5 h of acute right testicular pain after a game of football. He had experienced 6–7 similar episodes in the last 2 years where the pain had spontaneously resolved. Cremasteric reflex was absent on the right. (A) Gray-scale transverse US image of the right testis shows a redundant spermatic cord (arrow) occupying the medial half of the scrotal sac, with a mildly edematous epididymis (E) adjacent to it. The echogenic mediastinum testis faced medially instead of posterolaterally, which was concerning for altered testicular lie. (B) Color Doppler longitudinal image of the right scrotum shows excess and tortuous spermatic cord bunched up in the scrotal sac superior to the testis and formation of a pseudomass, suggesting torsion of the spermatic cord. Note that this extratesticular pseudomass is not hyperemic and should not be confused with epididymitis. Orchiopexy was recommended; however, the family chose to wait because his pain had improved. Elective orchiopexy was performed 7 months later and bilateral bell clapper anomaly was noted; he was diagnosed with intermittent torsion. (Image obtained from Bandarkar AN, Blask AR. Testicular torsion with preserved flow: key sonographic features and value-added approach to diagnosis. Pediatr Radiol. 2018;48(5):735–744. doi:10.1007/s00247-018-4093-0.Citation27 Distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/). No changes have been made to the images or the image description).
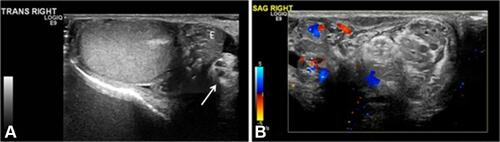
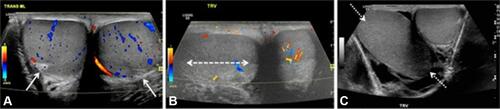
Figure 3 Testicular lie—normal and abnormal. (A) Color Doppler transverse US image of the testes in a 12-year-old boy with mild groin pain demonstrates normal vertical lie with the testes seen in round cross-section and with the mediastinum testis (arrows) directed posterolaterally. (B) Color Doppler transverse US image of both testes in a 14-year-old boy who woke with acute right scrotal pain demonstrates abnormal horizontal lie of the right testis (arrow) with slightly decreased intratesticular flow compared to the normal left side. He had experienced similar episodes of pain in the past and was diagnosed with intermittent torsion. During orchiopexy 12 h later, a bell clapper deformity was noted bilaterally. (C) Gray-scale transverse US image of both testes in a 16-year-old boy with right testicular pain demonstrates abnormal oblique lie of the right testis (arrows), which is oriented diagonally compared to the normal left side. Intermittent torsion was diagnosed intraoperatively. (Image obtained from Bandarkar AN, Blask AR. Testicular torsion with preserved flow: key sonographic features and value-added approach to diagnosis. Pediatr Radiol. 2018;48(5):735–744. doi:10.1007/s00247-018-4093-0.Citation27 Distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/). No changes have been made to the images or the image description).