Figures & data
Table 1 Data summary of the 12 patients who underwent our newly developed surgical method for punctal occlusion
Figure 1 Surgical steps of our newly developed punctal occlusion method ([A]. schematic diagram, [B]. surgical photo).
Notes: (1) diathermy, (2) deepithelialization with a hand-held motor burr grinder, (3) removal of a section of the medial rectus capsulopalpebral fascia (CPF) from under the lacrimal caruncle, (4) insertion of the CPF tissue into the deepithelialized canaliculus, (5) anchoring and additional sutures placed to fix the CPF tissue against the deepithelialized canalicular wall to close the punctum.
![Figure 1 Surgical steps of our newly developed punctal occlusion method ([A]. schematic diagram, [B]. surgical photo).](/cms/asset/edabe125-ac92-4dd7-87f3-f5bc1304108a/doph_a_155209_f0001_b.jpg)
Figure 2 Representative case in which puncta are clearly visible (Case 12 in ).
Note: Images showing the enlarged puncta due to frequent punctal-plug extrusion that appeared prior to the patient undergoing our newly developed surgical method (left, arrowheads) and at 6-months postoperative (right, arrowheads).

Figure 3 Changes in ocular parameters pre and post surgery.
Notes: (A) Tear meniscus radius (TMR). (B) Interference grade (IG). (C) Fluorescein breakup time (FBUT). (D) Fluorescein scores of area (FSA). (E) Fluorescein scores of density (FSD). (F) Lissamine green scores (LGS). *P<0.05, **P<0.01.
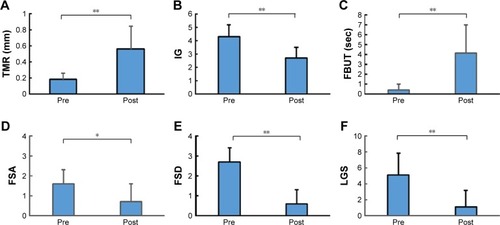
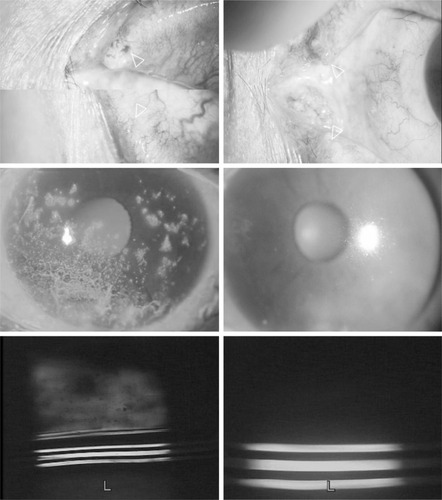
Figure 4 Representative case (Case 5 in ).
Notes: The left-side images show the condition of the eye prior to surgery. The top-left image shows the upper punctal plug completely extruded and hanging by sutures which were intended to fix it in the punctum. This patient experienced frequent punctal-plug extrusion in both the upper and lower puncta. The middle-left image shows the preoperative corneal epithelial damage (scored as A2D3). The bottom-left image was obtained prior to surgery by video-meniscometer (calculated tear meniscus radius [TMR]: 0.17 mm). The right-side images show the condition of the eye at 6-months postoperative. The top-right image shows the puncta completely closed after undergoing our new surgical method (arrowheads). The middle-right image shows the condition of corneal epithelial damage (scored as A1D1), and the bottom-right image shows increased tear volume, as evaluated by video-meniscometer (calculated TMR: 0.36 mm).
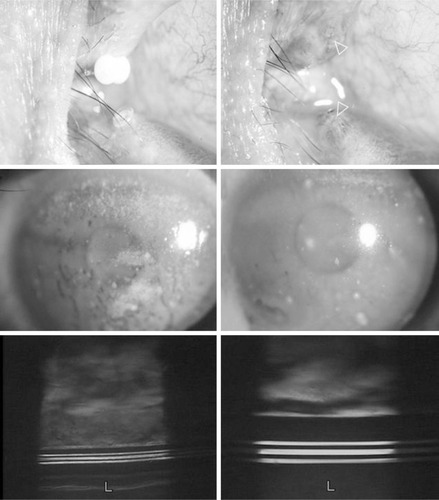
Figure 5 Representative case (Case 7 in ).
Notes: The upper and lower puncta of this patient had been unsuccessfully operated on four times by conventional methods of diathermy and suturing. The left-side images illustrate the preoperative condition. The top-left image shows that the upper punctum is enlarged (arrowhead) and that the lower punctum appears to have a tiny reopening (arrowhead) (Note: the upper and the lower punctum were photographed separately and adapted together for the punctum to be more clearly focused). The middle-left and bottom-left images show the condition of corneal epithelial damage (scored as A2D3) and the video-meniscometry photograph, respectively (calculated TMR: 0.33 mm). The right-side images show the condition of the eye at 6-months postoperative. The top-right image shows the puncta (arrowheads) being completely closed post our new surgical method. The middle-right image shows the condition of corneal epithelial damage (scored as A0D0), and the bottom-right image shows increased tear volume, as evaluated by video-meniscometer (calculated TMR: 0.88 mm).