
Figures & data

Figure 1 o-MGD classification diagram. The top row of images represents a fixed, firm, focal, unyielding resistance (FFFUR) with obstruction (indicated by the orange ring around the gland duct) of the meibomian gland (MG) distal to all acini. This type of obstruction will initially present with lid tenderness (LT), as meibum is being produced without an escape, leading to the build-up of pressure behind the obstruction (this obstruction is termed complete distal obstruction, or CDO, as depicted in the first image of the top row). Eventually, the build-up of pressure will result in a loss of function of the gland (termed complete distal obstruction non-functional, or CDO-NF, as depicted in the middle image of the top row), ultimately resulting in MG dropout as the entire gland atrophies (top row, right). No meibum will be expressed from this gland. The first two images in the bottom row represent a fixed proximal obstruction (indicated by the orange ring around the more proximal gland duct) of the MG, in which one or more acini are in communication with the central duct and orifice. LT will be present, as meibum is being produced without an escape, leading to the build-up of pressure behind the obstruction. However, this classification of MGs will have expressible meibum, as the acini located distally to the obstruction still remains in communication with the central duct and orifice (this obstruction is termed complete proximal obstruction, or CPO, as depicted in the first image of the bottom row). Eventually, the build-up of pressure will result in a loss of function of the gland proximal to the obstruction (CPO-NF). Without relief of obstruction, there would ultimately be significantly increased numbers of short, truncated MG (middle image, bottom row) showing proximal atrophy. The final classification of partial distal obstruction (or PDO, as depicted in the bottom row, right), is the result of a partial distally obstructed gland, such as orifice squamous metaplasia. This gland presents with no LT, as there is not a complete obstruction, and meibum is able to be expressed at the orifice. Reproduced with permission from Maskin SL. Intraductal meibomian gland probing: a paradigm shift for the successful treatment of obstructive meibomian gland dysfunction. In: Tsubota K, ed. Diagnosis and treatment of meibomian gland dysfunction. Tokyo, Japan: Kanehara & Co., Ltd; 2016:149-167.Citation7
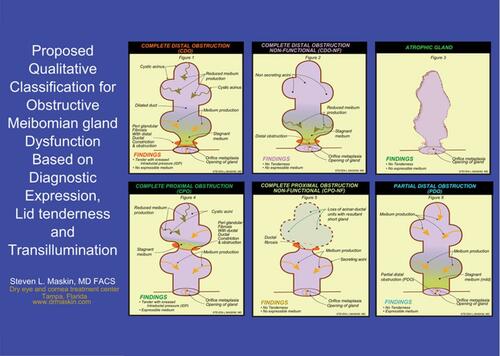
Figure 2 Release of occult trapped meibum along intraductal Meibomian gland probe and out through orifice after relief of a fixed, firm, focal unyielding resistance (FFFUR) type of obstruction. Reproduced with permission from Maskin SL. Intraductal meibomian gland probing relieves symptoms of obstructive meibomian gland dysfunction. Cornea. 2010;29(10):1145–1152 (https://journals.lww.com/corneajrnl/Abstract/2010/10000/Intraductal_Meibomian_Gland_Probing_Relieves.13.aspx).Citation4
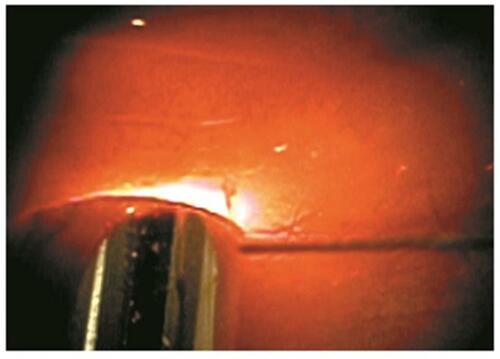
Figure 3 Our study results as seen in this graph show the dramatic and immediate resolution of lid tenderness (LT) in 86% of 144 lids within one-week post probing in patients with classification of CDO (LT with four or less glands per lid expressible) and CPO (LT with five or more glands per lid expressible). There was also a resolution of LT in 82% of 215 lids at 3–6 months and 58% of 113 lids at one-year follow-up. At each time point evaluated, results were stratified according to Meibomian gland atrophy using infrared meibography. Results showed that although those lids with less than 50% atrophy showed better results at each time point compared to lids with greater than 50% gland atrophy, this finding was not statistically significant. Maskin and Hethorn, unpublished data, 2015.
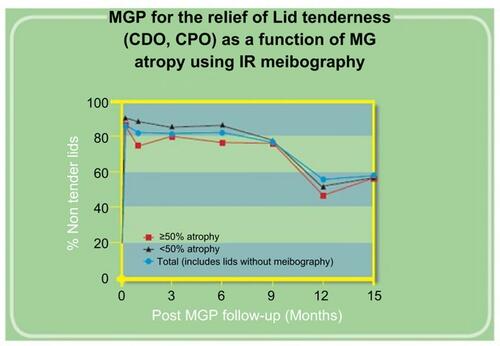
Figure 4 Our study results as seen in this graph show the rapid post probing restoration of meibum secreting lid functionality (MSLF) (at least five expressible glands per lid) to lids with pre-probing classification of CDO (four or less expressible glands per lid with lid tenderness) or CDO-NF (four or less expressible glands per lid without lid tenderness). There was a return of MSLF in 94% of 64 lids at 1week, 92% of 102 lids at 3–6 months and 74% of 46 lids at one-year follow-up. At each time point evaluated, results were stratified according to Meibomian gland atrophy using infrared meibography. Results showed that although those lids with less than 50% atrophy showed better results at each time point compared to lids with greater than 50% gland atrophy, this finding was not statistically significant. Maskin and Hethorn, unpublished data, 2015.
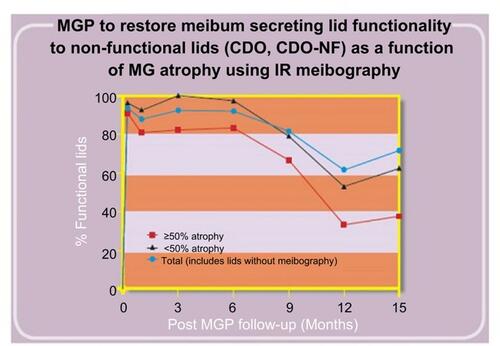
Figure 5 Our study results as seen in this histogram show the increase in numbers of expressible glands per lid after probing. All 25 lids showed four or less expressible glands per lid pre-probing with an average of 2.80 while at a mean follow up of 2.45 months showed 14.36 expressible glands per lid, an increase of 412%. Maskin, unpublished data, 2018.
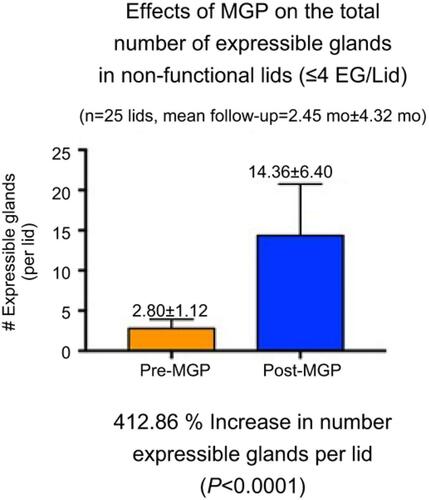
Figure 6 Clinical exam findings post probing: Pre-probing photo, (A) shows the appearance of left upper lid with lid margin vascular engorgement and gland plugging; (B) is 2 months after gland probing showing vessel regression with a marked reduction in vascular caliber and gland plugging. There was an associated marked reduction in lid tenderness visual analog scale (VAS) from the pre-probing score of 45 out of 100 to his latest score of 0 at 23 months post probing. The lid showed intact meibum secreting functionality with more than 10 glands showing expressible meibum. Reproduced with permission from Maskin SL. Intraductal meibomian gland probing: a paradigm shift for the successful treatment of obstructive meibomian gland dysfunction. In: Tsubota K, ed. Diagnosis and treatment of meibomian gland dysfunction. Tokyo, Japan: Kanehara & Co., Ltd; 2016:149–167.Citation7
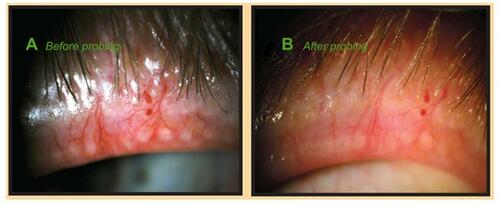
Figure 7 Post probing example of increased Meibomian gland tissue area on infrared meibography: The rectangles in (A–C) highlight the atrophic area in the TMF where growth has occurred. (A). Pre and post probing image capture from IR meibography video. (B) Pre and post probing image capture after being processed through Adobe Photoshop simply to desaturate and invert the color image. (C) Pre and post probing traces of the total measurement field (TMF), and each individual meibomian gland (MG). The pre-probing images show proximal atrophy with shortened gland length. Post probing shows an increased lengthening of these glands. (D) Statistical analysis revealed a significant increase in glandular tissue post probing (t=5.947, p=0.0001), representing a 19.93% growth in total MG tissue area. Reproduced from Growth of meibomian gland tissue after intraductal meibomian gland probing in patients with obstructive meibomian gland dysfunction, Maskin SL, Testa WR, 102, 59-68, Copyright © 2018, with permission from BMJ Publishing Group Ltd.Citation3
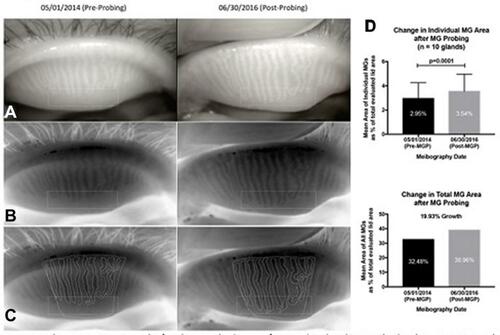
Table 1 Review of literature for meibomian gland probing
Figure 8 Case study of probing for a 66-year-old woman with obstructive MGD (upper lid): (A) before probing, the left upper lid had 0 expressible glands and VAS showed 44 out of 100 scale for tenderness for a diagnosis of complete distal obstruction (CDO), while 1 week after probing (LU After); (B) the same lid had more than 10 expressible glands and VAS showed 7 of 100 in tenderness for a diagnosis of partial distal obstruction (PDO). Reproduced with permission from Maskin SL. Intraductal meibomian gland probing: a paradigm shift for the successful treatment of obstructive meibomian gland dysfunction. In: Tsubota K, ed. Diagnosis and treatment of meibomian gland dysfunction. Tokyo, Japan: Kanehara & Co., Ltd; 2016:149–167.Citation7
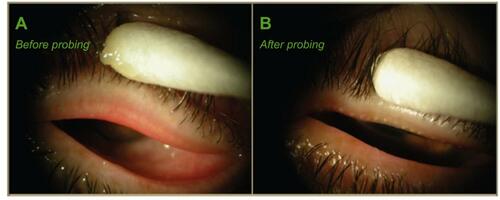
Figure 9 Case study of probing of lower lid for patient in : (A) before probing, the left lower lid had 0 expressible glands and VAS of 47 of 100 tenderness for diagnosis of CDO, while 1 week after probing (LL After); (B) the same lid had more than 10 expressible glands and VAS showed 0 of 100 tenderness for a diagnosis of PDO. Reproduced with permission from Maskin SL. Intraductal meibomian gland probing: a paradigm shift for the successful treatment of obstructive meibomian gland dysfunction. In: Tsubota K, ed. Diagnosis and treatment of meibomian gland dysfunction. Tokyo, Japan: Kanehara & Co., Ltd; 2016:149–167.Citation7
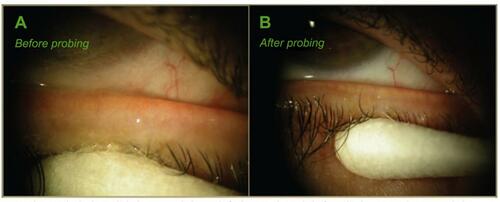
Table 2 Case study of meibomian gland probing