
Figures & data
Figure 1 Skin and muscle surgery: (A) Skin incision was done 3–4 mm away from the lid margin covering the lateral 2/3 of lid width. (B) Incision in the orbicularis muscle (muscle layer) was made. A strip of orbicularis oculi was excised. (C) Closure of the muscle layer with 6/0 Coated VICRYL (interrupted stitches) was done. Closure of the skin with continuous 6/0 Coated VICRYL was done.
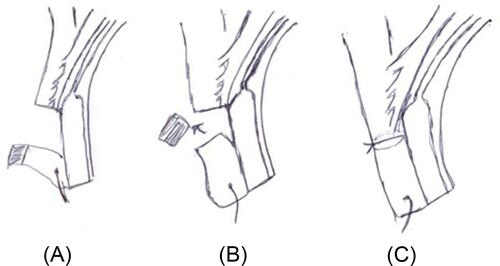
Figure 2 Lamellar tarsectomy procedure: (A) The pretarsal orbicularis fibers and the anterior fibers of the muscle of Riolan were divided till visualization of the external surface of the tarsus. Two lines in tarsal surface in a distance 2–3 mm in between were marked with superblade 30 degrees (MANI-MST-30), deep incisions. (B) D-shaped lamellar incision of external surface of tarsus was made to remove the superficial lamella of tarsus with groove formation. (C) Three 6/0 Coated VICRYL stitches were taken from the peripheral incision line to the anterior incision line without cutting the tarsus. As the sutures were tied, the lid margin might rotate outward, causing the lashes to rotate externally away from the cornea.
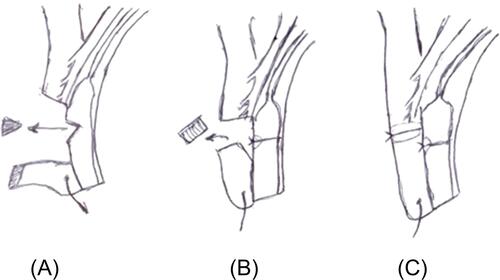
Figure 3 Lamellar tarsectomy procedure, groove formation with removal of the superficial lamella of tarsus and starting the tarsal rotating sutures.

Table 1 Baseline Demographic And Clinical Characteristics Of Patients In Both Groups Of The Study
Table 2 Trichiasis Status Of Participants In Each Group Of The Study At 6 And 12 Months
Figure 4 Cumulative survival analysis revealed early vertical sloping (failure 6 weeks after surgery) in the skin and muscle surgery group (blue curve; success rate 60%), and late vertical sloping (failure 3 months after surgery) in the lamellar tarsectomy group in (green curve; success rate 90%).
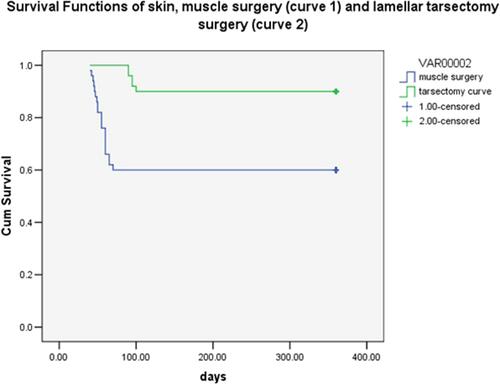
Table 3 Clinical Characteristics Of Participants In Each Group Of The Study At 12 Months
Table 4 Symptoms And Complications Reported By Participants At 12-Months Follow-Up