
Figures & data
Figure 1 Flowchart of diagnostic approach in suspected ocular fungal infection.
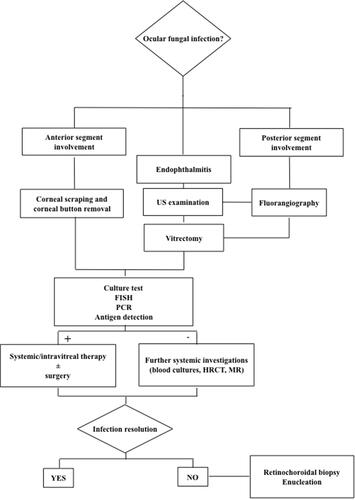
Figure 2 Biomicroscopic examination of Aspergillus corneal infection. (A) 4 days after penetrating keratoplasty (PKP) for keratoconus: intense perikeratic reaction, mild corneal edema, Descemet folds, “mutton fat” endothelial keratic precipitates and anterior chamber flare. Whitish wax-like material is visible behind the pupil. (B) 6 days after PKP: large central epithelial defect with perikeratic injection, dense whitish infiltrates and a stromal melting started from the edge of the donor graft. (C) 9 days after PKP: diffuse stromal melting, the donor graft is raised in the lower sector. (D) 3 months from repeated PKP: clear corneal graft, well-stretched sutures and no signs of inflammation.
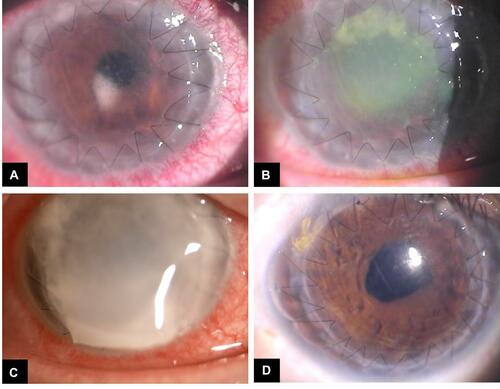
Figure 3 Fundus retinography of Aspergillus infection involving the posterior segment: subretinal exudates, intraretinal hemorrhages spread into the retina extended to the posterior pole.
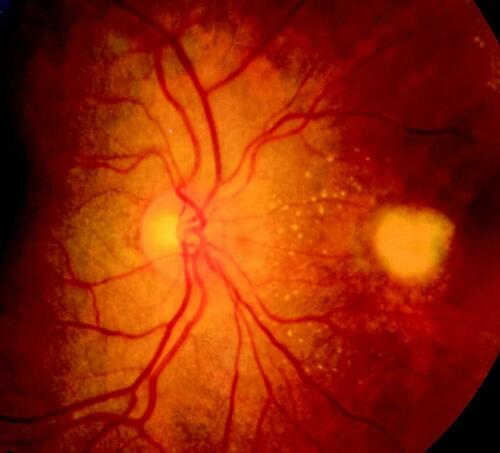
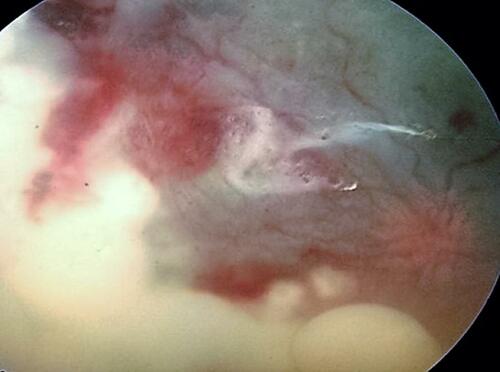
Figure 4 Fundus retinography of Aspergillus endophthalmitis showing vitritis, dense and wide white-yellow creamy lesions, diffuse intraretinal hemorrhages, partial retinal detachment.
Box 1 Major Effects of Ocular Involvement by Aspergillus