
Figures & data
Figure 1 The right eye from the surgeon’s perspective depicting pupillary miosis and a dense, mature cataract. A standardized technique was used to create a continuous curvilinear capsulorhexis (CCC). (A): 1mm corneal paracentesis. (B): Methylparaben free xylocaine was injected intracamerally to numb the iris then cohesive viscoelastic was used to fill the anterior chamber. (C): 2.4mm temporal clear corneal incision with a microkeratome blade. Posterior synechiae, if present, were broken with a collar button. (D): A 6.25mm malyugin ring was placed to expand the pupil. (E): Cohesive viscoelastic was then removed via an irrigating/aspiration tip. (F): A small amount of viscoelastic was then used to seal the paracentesis. A 27-gauge cannula was then used to inject air through the paracentesis. If air was leaking through the temporal corneal wound, a temporary single 10–0 nylon could be placed in the incision. (G): Trypan blue was then injected through the paracentesis to stain the anterior capsule. (H): The air bubble and trypan blue were subsequently removed by filling the anterior chamber with a dispersive viscoelastic through the paracentesis. (I): The 10–0 nylon suture was removed from the temporal incision if it was previously placed. A ~5mm CCC was initiated with a cystotome and completed using Utrata Forceps.
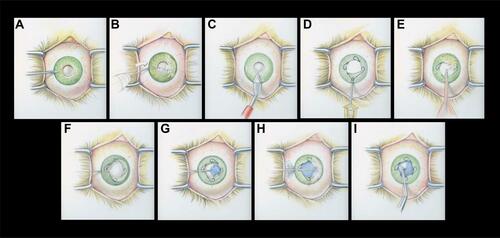
Table 1 Patient Demographics, History, and Cataract Grade
Table 2 Surgical Outcomes and Mechanism for Miosis