Figures & data
Table 1 Patient Demographics and Clinical Features
Table 2 Clinical Findings on Multimodal Imaging at Diagnosis and During Follow-Up
Figure 1 Clinical features visible on multimodal imaging of the left eye of a 37-year-old male patient with aCSC. (A) Color fundus photograph showing small pigment clustering in the macula and a silhouette of the serous retinal detachment. The arrow indicates the scanning plane, which is depicted on the SD-OCT. (B) FAF image at diagnosis showing a speckled (ie, granular) hyper-autofluorescent lesion at the site of the serous neuroretinal detachment. (C) FA imaging revealed a single “hot spot” of leakage and a typical small detachment of the RPE above the inferior retinal arcade (arrow). (D) An SD-OCT scan at diagnosis revealed SRF accumulation, a thickened choroid, and subretinal debris, presumably consisting of non-phagocytized photoreceptor outer segments. (E) SRF resolved spontaneously within a few weeks. (F) The areas of hyper-fluorescence on mid-phase ICGA revealed diffuse choroidal hyperpermeability that was larger than the leakage site visible on FA. A recurrent episode 1.5 years later was treated with two subthreshold micropulse diode laser but did not result in resolution of the SRF. Eventually, half-dose photodynamic therapy resulted in resolution of the SRF (G and H). At the patient’s final visit 11 months later, hyper-autofluorescent and hypo-autofluorescent abnormalities were visible (G), and FA imaging revealed a slightly enlarged area of RPE alterations (H).
Abbreviations: aCSC, acute central serous chorioretinopathy; ICGA, indocyanine green angiography; FA, Fluorescein angiography; FAF, Fundus autofluorescence; SD-OCT, spectral-domain optical coherence tomography; SRF, subretinal serous fluid; RPE, retinal pigment epithelium.
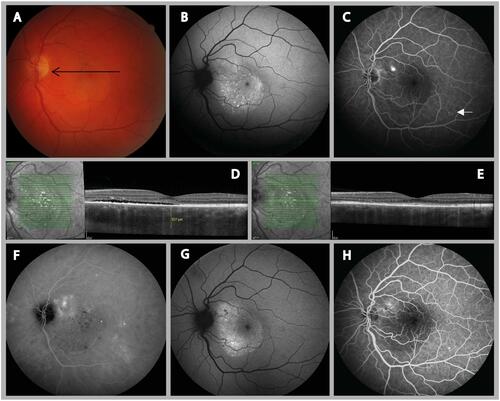
Figure 2 Clinical features visible on multimodal imaging of the right eye of a 37-year-old female patient (A–D) and a 34-year-old male patient (E–H) with aCSC. (A and E) FA revealed one focal “hot spot” of leakage and no changes in the retinal pigment epithelium. (B and F) Despite these circumscribed lesions on FA, ICGA revealed a more widespread area of hyper-fluorescence, which corresponded with multifocal (B) or monofocal (F) choroidal leakage. (C and G) FAF imaging revealed speckled (ie, granular) hyper-autofluorescent changes at the site of serous neuroretinal detachment in both patients, which corresponded with serous retinal detachment visualized on OCT (D, H).
Abbreviations: aCSC, acute central serous chorioretinopathy; ICGA, indocyanine green angiography; FA, Fluorescein angiography; FAF, Fundus autofluorescence; OCT, optical coherence tomography; SRF, subretinal serous fluid; RPE, retinal pigment epithelium.
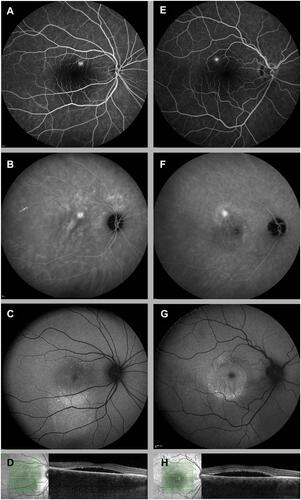
Table 3 Treatment Modalities and Specifications During Follow-Up in Patients with Acute CSC
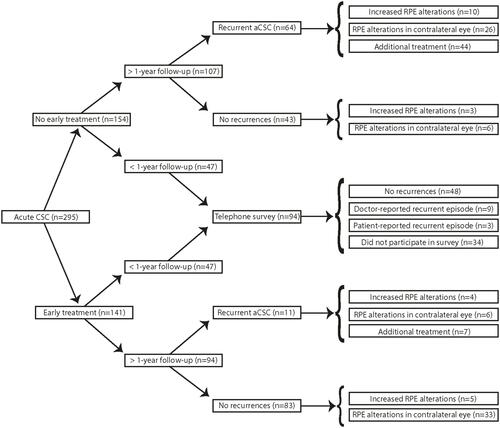
Figure 3 Flow chart depicting the distribution of the eyes in this study, with follow-up durations indicated. The development of CSC over time is based on recurrence of the disease, progression of RPE alterations, and the need for additional treatments.
Abbreviations: CSC, cute central serous chorioretinopathy; RPE, retinal pigment epithelium.