
Figures & data
Table 1 Preoperative Status
Table 2 Procedure for Lens Extraction and Vitrectomy
Figure 1 Port-fixation group. Representative case, right eye. (A)Supranasal (c) and inferotemporal (b) trocars (25-gauge) were placed in the center of a T-shaped lamellar scleral incision 2 mm from the corneal limbus and a supratemporal trocar (a) was placed 3.5 mm from that. (B, C) Following a vitrectomy, the infusion cannula was changed from an inferotemporal to supratemporal trocar. At the time when the IOL was halfway inserted into the eye (d), the first IOL haptic and a supranasal trocar were simultaneously withdrawn through the sclera by grasping with 25-gauge vitreoretinal forceps. (D, E) The second IOL haptic and an inferotemporal trocar were simultaneously withdrawn through the sclera by grasping with 25-gauge vitreoretinal forceps. (F) Both tips of the IOL haptics were embedded into preliminary intrascleral spaces and the infusion cannula was finally removed.
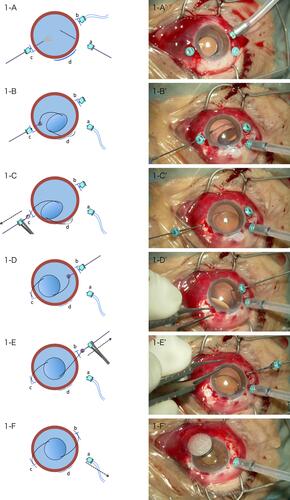
Figure 2 Conventional group. Representative case,righteye. (A) Supratemporal (a),inferotemporal (b) and supranasal (c) trocars (25-gauge) were placed 3.5 mm from the corneal limbus. Two T-shaped lamellar scleral incisions were placed 2 mm from that (e,f). In the center of T-shaped lamellar scleral incisions,full-thickness scleral perforations were performed with 25-gauge MVR. (B,C) Following a vitrectomy,IOL was halfway inserted into the eye (d) and the first IOL haptic was withdrawn through the scleral perforation site (f) by grasping with 25-gauge vitreoretinal forceps. (D,E) The second IOL haptic was withdrawn through the scleral perforation site (e) by grasping with 25-gauge vitreoretinal forceps. (F) Both tips of the IOL haptics were embedded into preliminary intrascleral spaces (e,f),and two trocars (a,c) and the infusion cannula were finally removed.
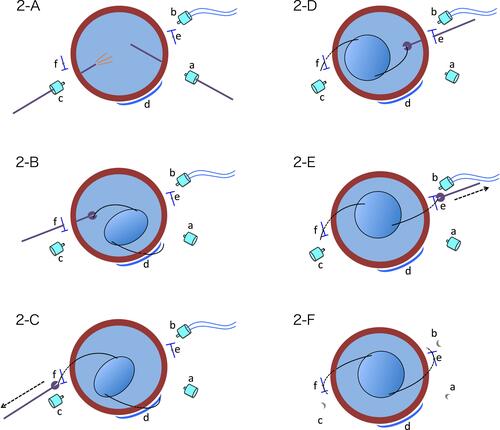
Table 3 Postoperative Complications, Pre- and Postoperative Visual Acuity