
Figures & data
Figure 1 This is a SS-OCT of a normal left eye of a 45-year-old female. The blue arrow on the color fundus photograph indicates the position of the OCT B-scan. The yellow arrow indicates a Haller vessel, the blue arrow a Sattler vessel, and the red arrow the choriocapillaris, a 10–30 micron thick layer immediately subjacent to the Bruch’s membrane. The choroidal thickness varies greatly from person to person, by location relative to the optic nerve and fovea, over time with aging, and in diseases such a central serous retinopathy (thicker than normal) and high myopia (thinner than normal). In the case shown here, the choroid is thicker between the fovea and optic nerve (white double headed arrow) than at the fovea (purple double headed arrow), and thinner nearer the optic nerve (double headed green arrow).
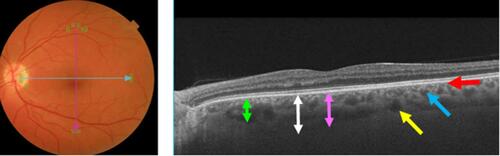
Figure 2 Red free photograph (top) and spectral domain OCT image (bottom) from the left eye of a 68-year-old man with pathologic myopia and a previously undescribed variant of macular intrachoroidal cavitation. The lesion occurs in an area of RPE and choroidal atrophy in an area of excavation of the thickened subjacent sclera producing a pseudofovea of a sort different from that described in macular intrachoroidal cavitation.
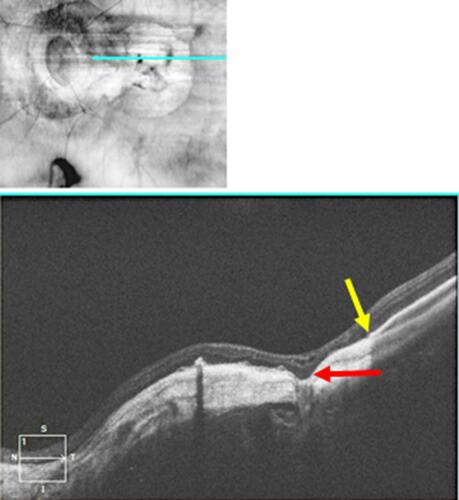
Figure 3 Near infrared reflectance image (left panel) and B-scan OCT image (right panel) of a 68-year-old woman with pathologic myopia. The scleral thickness varies widely (compare the red double-head arrows in nasal and temporal macula, respectively). Where the sclera thins and bows outward, the choroid thickens (space between the two yellow arrows) compared to the choroidal thickness overlying thick sclera (space between two green arrows). However, instead of a choroidal cavitation, the associated response seen is outer nuclear layer retinoschisis (purple arrow). The blue arrows indicate a large intrascleral vein.
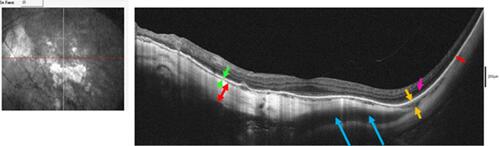
Figure 4 SD-OCT of conforming FCE in the macula shows the outer retinal layers in apposition to the area of focal choroidal concavity.
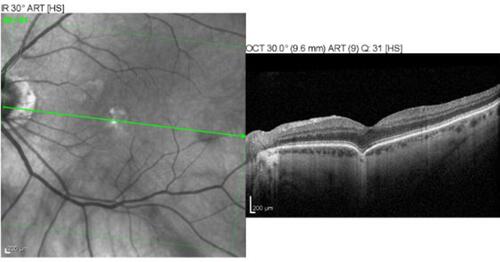
Figure 5 SD-OCT of non-conforming FCE in the macula. In contrast to the conforming type FCE in , non-conforming shows a separation of photoreceptor tips from RPE.
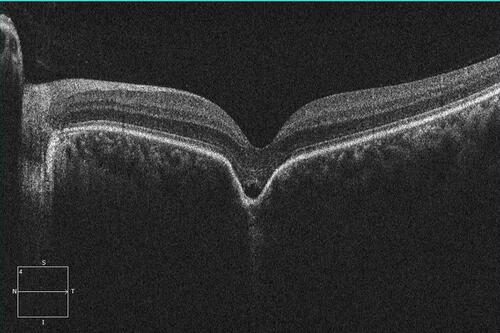
Figure 6 SD-OCT image of a patient with nonexudative AMD in which a PED developed with focal atrophy of the RPE at the crest of the PED (red arrow), but in which the Bruch’s membrane remained intact (yellow arrow). The subjacent choroid (blue oval) suffered no choroidal excavation. Destruction of the Bruch’s membrane is hypothesized to be a necessary precondition for FCE development in acquired cases.
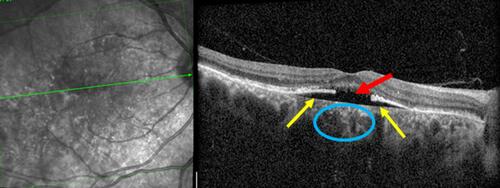
Figure 7 Color fundus photograph (A) near infrared reflectance image (B), and SD-OCT image (C) of an 8-year-old girl with torpedo maculopathy of the right eye. Her visual acuity was 20/20 bilaterally. The fovea is spared. The point of the torpedo lesion is closest to the fovea. The lesion would be classified as type 2 because of the cavitation (green arrow) of the outer retina. The outer nuclear layer over the cavitation (pink arrow) is attenuated. The choroid is attenuated, but the scleral-choroidal interface is not affected (yellow arrows). The retinal pigment epithelium at the base of the outer retinal cavity is hypopigmented in the color fundus photograph and hyporeflective in the OCT image.
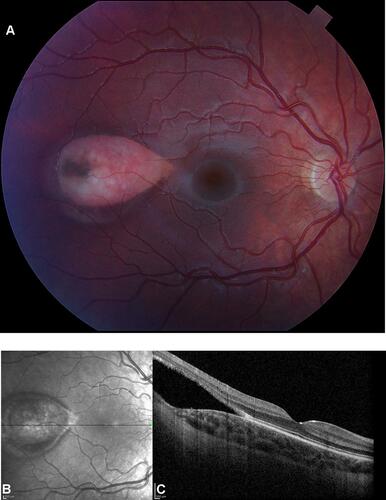
Table 1 Choroidal Cavitary Disorders Summary