Figures & data
Figure 1 Schematic of the first-generation Kahook Dual Blade (KDB) on the left and the second-generation KDB Glide on the right illustrating new design features with a comparison overlay image (center), including beveled edges and rounded corners (red) at the bottom of the second-generation device to enhance passage through the Canal of Schlemm. The ramp and dual blade dimensions and design elements are conserved between the two devices.
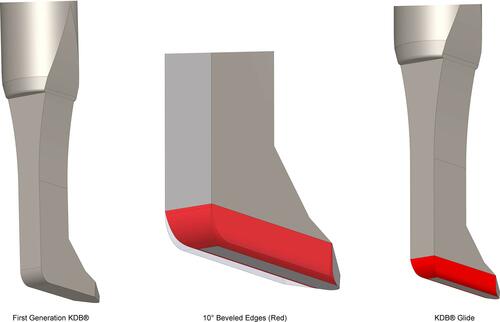
Figure 2 TrabEx blade, featuring two serrated blades (arrow) without a non-cutting ramp.

Figure 3 Histology of the intact human anterior chamber angle showing the remnant of the iris (IR), the Canal of Schlemm (SC), and the trabecular meshwork (arrow). H&E stained sections, scale bar = 200 µm.
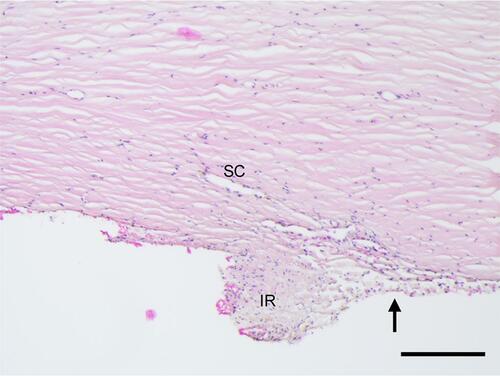
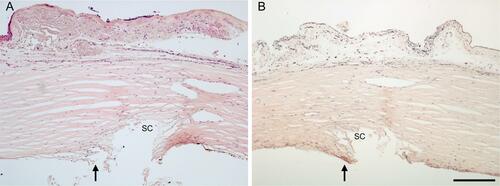
Figure 4 The anterior chamber angle following MVR goniotomy created an incision in the trabecular meshwork (TM) without removal of TM leaflets (arrows), through the Canal of Schlemm and passing to varying depths into the scleral wall (SW). In (A), the incision extended deep into the scleral wall and a visible ~200 µm remnant of TM is apparent (arrow). In (B) the incision extends just past the outer wall of the Canal of Schlemm, also showing no excision of TM (arrows). H&E stained section, scale bar = 200 µm.
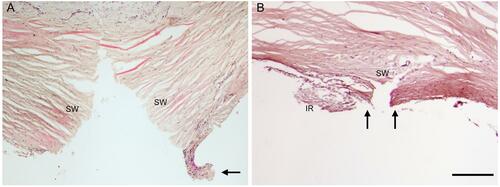
Figure 5 The anterior chamber angle following 360° Trabeculotomy resulted in incision through the trabecular meshwork (TM) proximate to Schwalbe’s line with no evident excision of TM leaflets. The arrows in (A and B) indicate large TM flap leaflets in two distinct sections of treated tissue. There is no apparent damage to the outer wall of the Canal of Schlemm in the treated areas. H&E stained section, scale bar = 200 µm.
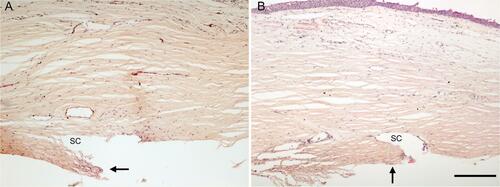
Figure 6 The anterior chamber angle following TrabEx goniotomy showed partial removal of trabecular meshwork with large leaflet tissue remnants (ranging from 100–200 µm in length, arrows) over the Canal of Schlemm (SC) in both (A and B). H&E stained sections, scale bar = 200 µm.
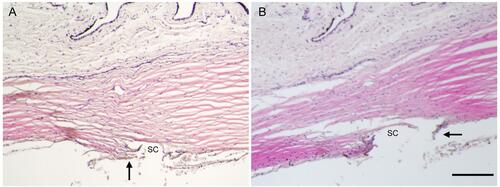
Figure 7 The anterior chamber angle following KDB Glide goniotomy showing near-complete excision of TM overlying the Canal of Schlemm (SC) in both (A and B) with minimal leaflet tissue remnants (ranging from 0 to 50 µm, arrows). H&E stained sections, scale bar = 200 µm.