Figures & data
Table 1 Clinical Activity Score (CAS)
Table 2 Classification of the Severity of Graves’ Orbitopathy (GO)
Figure 1 MRI findings of GO with DON (T2-weighted and fat-suppressed images using short-tau inversion recovery (STIR) sequences). Right: extraocular muscle swelling in both orbital cavity/. Left: extraocular muscle swelling compressing the optic nerve around the common tendinous ring.
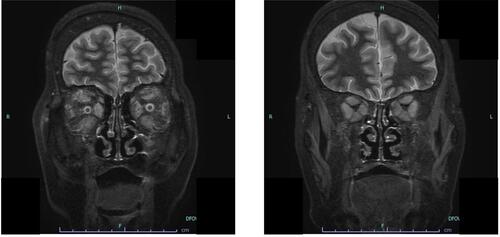
Figure 2 Algorithm for the management of sight-threatening Graves’ orbitopathy including DON. The first-line treatment for optic neuropathy is high-dose IV methylprednisolone or steroid pulse therapy (single doses of 500 to 1000 mg) for three consecutive days, or preferably and for safety reasons, every second day (alternate days) during the first week, which can be repeated for a second week. When the response is absent or poor, with deterioration in visual acuity or CFF, urgent orbital decompression surgery will be needed. Data from Bartalena L, Kahaly GJ, Baldeschi L, et al. The 2021 European Group on Graves’ orbitopathy (EUGOGO) clinical practice guidelines for the medical management of Graves’ orbitopathy. Eur J Endocrinol. 2021;185(4):G43–G67.Citation19
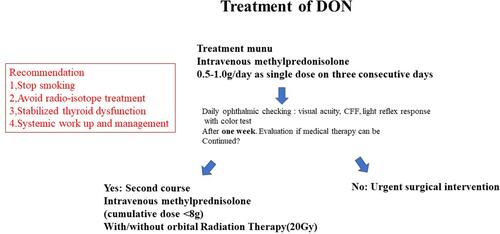
Figure 3 Schema of this review: Summary.