
Figures & data
Figure 1 The normal extent of the anterior segment captured with SS-OCT technology in one frame.

Figure 2 In a mature senile cataract, lenticular imaging on a modified OCT shows the presence of horizontal hypoechoic areas within the anterior cortex. It can also be noted that there is no collection of liquefied material in the lens and the anterior lens curvature is normal. This is the stage of early lamellar separation.

Figure 3 In the next stage of mature cataract, the separation becomes more advanced with little collection of liquefied material and minimal anterior lens bulging. This is the stage of established lamellar separation.

Figure 4 In the most advanced stage, a major portion of the anterior lens framework is lysed; hence, with subsequent collection of liquefied material, the anterior capsule bulges forward. This stage indicates extensive collection of liquefied material and raised intrabag pressures, which harbour the risk of capsule-related complications. This is the stage of liquefaction.

Table 1 ASOCT-Noted Observations Among Mature/Hypermature/White Cataracts
Figure 5 In a moderately dense cataract, posterior cortical and capsular details are better appreciated on cross-sectional imaging.
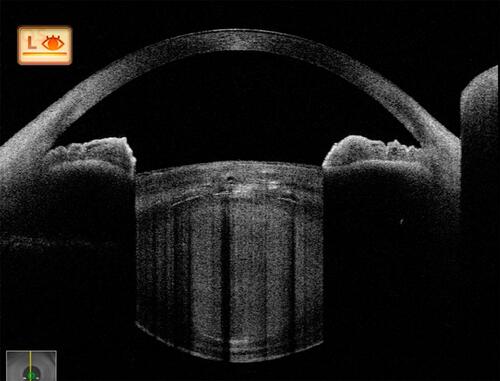
Table 2 Studies Highlighting the Role of ASOCT in Traumatic Cataracts
Figure 6 In a traumatic cataract with globular lens, its morphology, intralenticular changes, anterior subcapsular collection and a possible posterior defect are noted. The posterior defect needs to be further assessed on ImageJ software or MATLAB software with increased brightness and reduced background noise so as to clarify further its intactness.
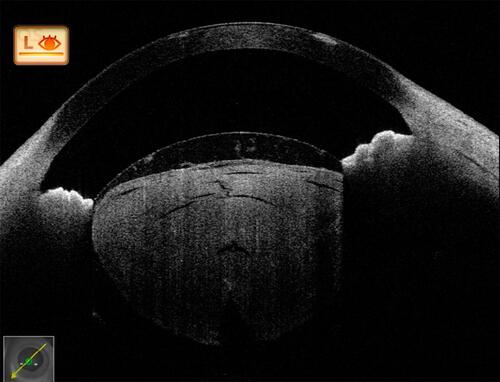
Figure 7 Post-traumatic cataract with partially absorbed lens matter showing a ruptured anterior capsule and matter spilling over into the anterior chamber. Again, here, in the presence of anterior dense opacity, posterior capsular details are very well appreciated before surgery.
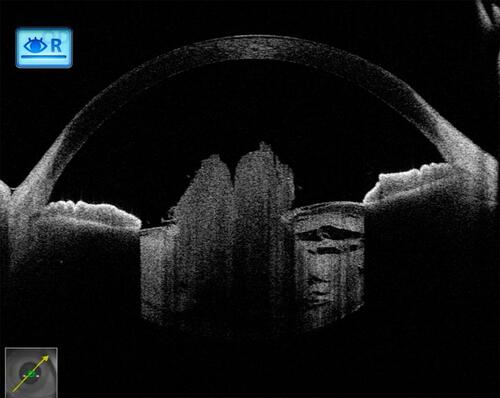
Figure 8 In a traumatic case, in its anterior portion, the anterior capsular flattening (white arrows) and cortical matter desiccation (red star) (A) can be appreciated. In further deeper scans, continuously appreciable intact posterior capsule (green arrows) (B), and an intact (green arrow) as well as discontinuous (red arrow) posterior capsule can be appreciated (C and D), with active herniation of cortical matter.
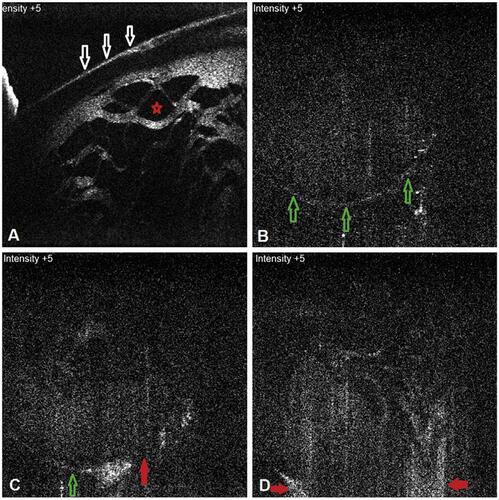
Figure 9 (A) In another two cases, posterior capsular dehiscence can be appreciated as posterior elongation of the torn capsule with active herniation of cortical matter (red arrows) (A, B).
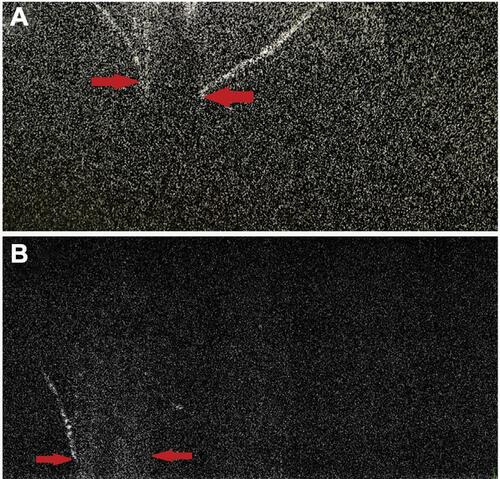
Figure 10 Four ASOCT images of posterior polar cataracts showing a definite dearth in posterior capsular continuity with active herniation of cortical matter into anterior vitreous (red dots). The consistent nipple-shaped configuration in these four images simulates a conical appearance (hence the conical sign) suggestive of posterior capsular deficiency.
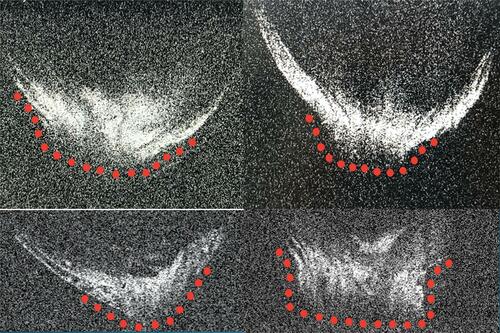
Figure 11 In a posterior polar cataract, posterior capsular deficiency with herniation of lens matter into anterior vitreous can be configured as the conical sign.
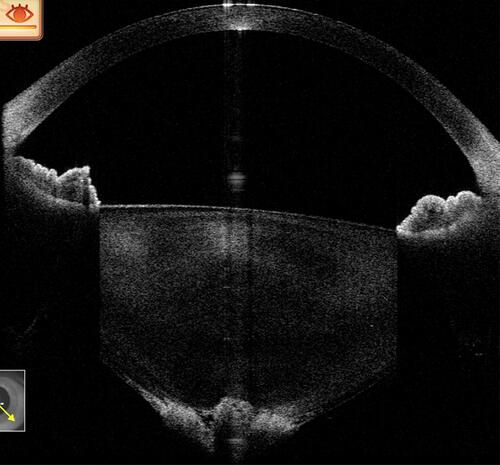
Figure 12 In another posterior polar cataract, the posterior lenticular appearance with deficient capsule can be configured as a moth-eaten appearance.
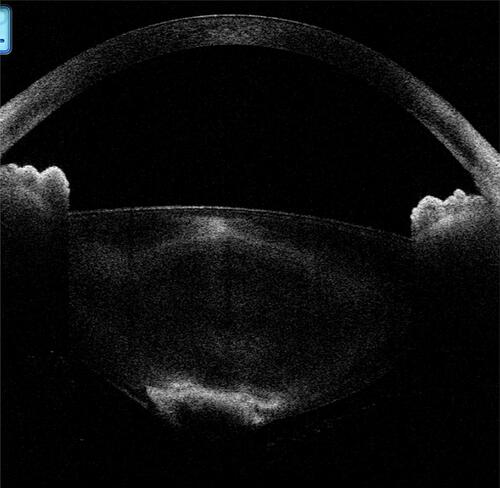
Figure 13 In a posterior polar cataract, the presence of hypoechoic areas between the capsule and the opacity can be configured as a with-hypoechoic variant. (It should be noted that several other complicated variants of this type exist, and for better understanding a simpler variant has been shown here.)
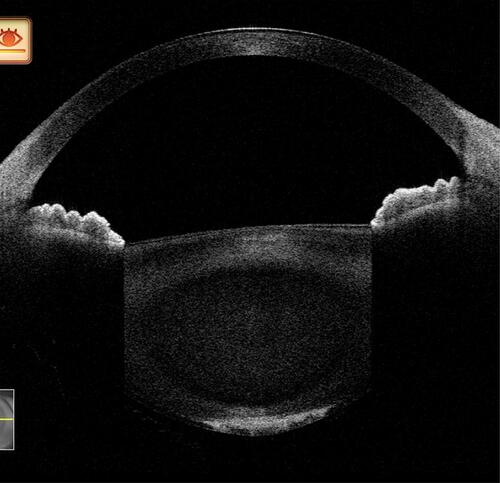
Figure 14 In a posterior polar cataract, the absence of hypoechoic areas between the opacity and the capsule can be configured as a without-hypoechoic variant. (It should be noted that several other complicated variants of this type exist, and for better understanding a simpler variant has been shown here.)
Table 3 ASOCT Studies on Posterior Polar Cataracts in Identifying the Deficient Posterior Capsule
Figure 15 A +20 lens mounted along the aperture of posterior segment OCT using a micropore tape. This will enable anterior segment imaging from the corneal surface to the posterior capsular tip (although not in one frame).
