Figures & data

Figure 1 Timeline for the Alaska OCR Study. Dates on left side including oldest Mayo Clinic and Indiana University (IU) studies. Publications listed to the right side with heart rate response during retinopathy of prematurity (ROP) examinations to lower right. Numbers studied at the bottom.
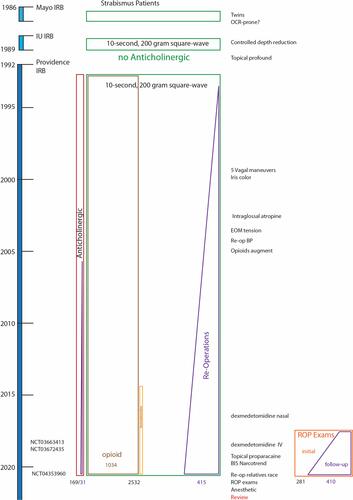
Figure 2 Uniform elicitation of oculocardiac reflex: anesthesiologist records anesthetic parameters and electrocardiograph stable pre-tension heart rate and then maximally altered heart rate as a response to the surgeon’s gentle isolation of an extraocular rectus muscle and then utilizing a sterile tension gauge passed through a hole in a Jameson hook and applying a 10-second, 200 gram square wave tension on the EOM tendon. (The individuals in this image all gave written consent to share for educational purposes).

Figure 3 Frequency Distribution; %OCR is defined as the maximally changed heart rate as a percent of stable baseline heart rate so bradycardia is to the left, tachycardia to the right and 100% representing no -change. OCR due to retinopathy of prematurity (ROP) exams on top compared with those due to 10-second, 200-gram square wave tension on a gently isolated (rectus) extraocular muscle (EOM) during routine, outpatient strabismus surgery. The median, interquartile range (box) and 95% limits (whiskers) for various influencers shown below. Green indicates more bradycardia and red indicates less bradycardia.
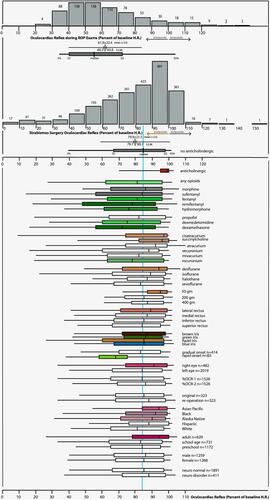
Figure 4 Neuroanatomy of the oculocardiac reflex. Trigeminal nerve afferents including extraocular muscle proprioceptors travel from the first division of the trigeminal nerve to be processed in the brain stem with efferent the cardiac vagus nerve.
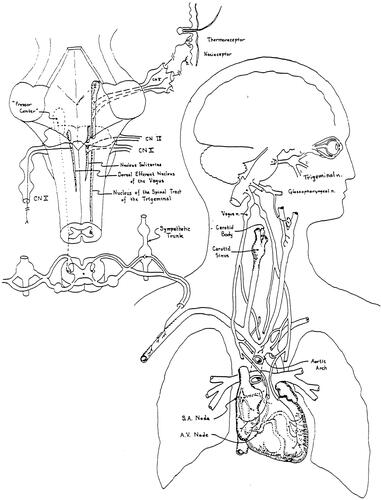
Figure 5 Cumulative Prevalence and past proportions. Curve fit for prevalence of %OCR versus degree of OCR (top) for adults and children undergoing 10-second, 200 gram square wave tension on rectus extraocular muscle (EOM). Bottom shows the compared cumulative prevalence including published studies that report OCR defined as 10% or more OCR (blue arrow), 20% or more OCR (red arrow) and profound 50% or more heart rate drop (green arrow).
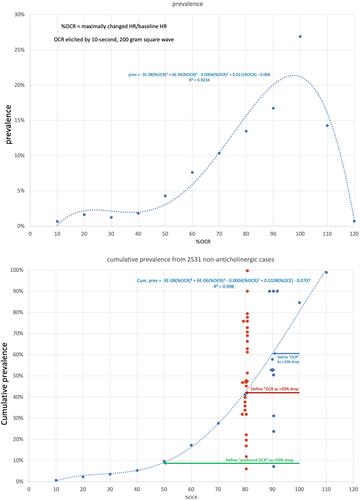
Figure 6 Extremes in oculocardiac reflex. From the Alaska OCR study: (A) influence of I.V. push remifentanil versus none. (B) Profound OCR. (C) Narcotrend brainwave monitor and profound OCR. (D, E and F) Multiple EOM tension during each case. (G) OCR with 20 second R-R interval repeat with Jameson muscle hooks and OCR tension gauge. (H) OCR with healthy adult athletic baseline heart rate rapidly showing 22 second R-R interval elicited by 10-second, 200 gram square wave tension on the inferior rectus muscle. (I) Oculocardiac reflex electrocardiograph and arterial pressure.
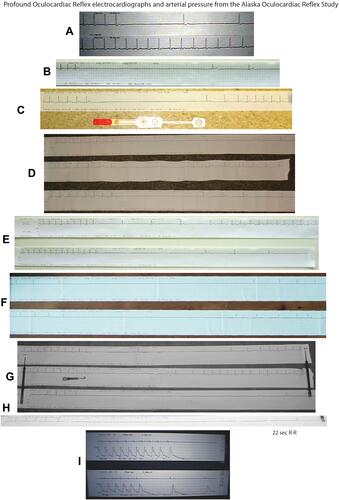
Figure 7 Influence of agent concentration (depth of anesthesia). The %OCR correlated with end-tidal concentration of inhaled anesthetic agent showing significantly less %OCR for deeper levels of agent for sevoflurane, halothane and isoflurane, but insufficient numbers of desflurane patients.
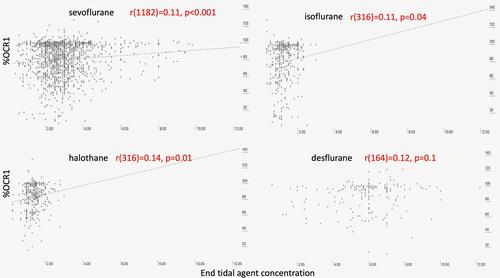
Figure 8 Influence of CO2 concentration. There is a trend toward more bradycardia due to OCR with hypercarbia.
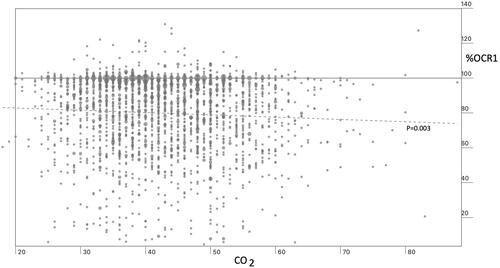
Figure 9 Laterality. The Alaska OCR study on two-eye cases usually performs the left eye first. For bilateral recordings, first eye, and also second eye had more %OCR with the left eye, but this also was true for cases with only one-eye surgery.
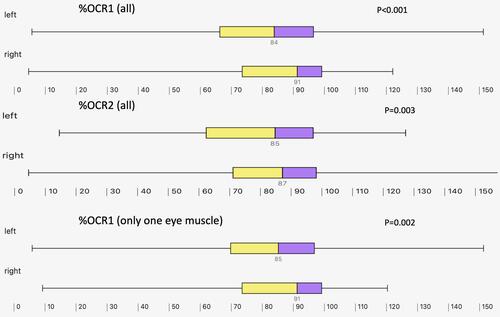
Figure 10 The correlations between the time interval between induction and EOM tension for first and second measurements of OCR produced by 10-second, 200 gram square wave tension on rectus muscles. OCR is presented as percent of stable, pre-tension heart rate. First muscle cases indicated with blue circles and blue linear correlation while second muscle cases are shown in orange diamonds with orange linear regression.
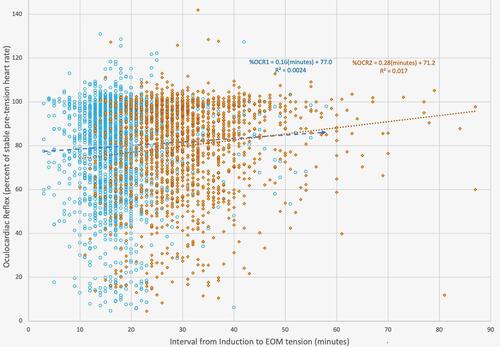
Figure 11 Influence on OCR by neurologic disorder: box (interquartile range with median in the middle and whisker (95 percentiles) of %OCR for patients with various neurologic conditions from the Alaska OCR study. ADHD is attention deficit hyperactivity disorder, CP is cerebral palsy, CVA is stroke, FAS is fetal alcohol syndrome, ICP in elevated intracranial pressure, ONH is optic nerve hypoplasia, Premi is marked prematurity less than 2000 grams birthweight, TBI is traumatic brain injury, move disorder is myasthenia gravis or multiple sclerosis, y is any neurologic disorder.
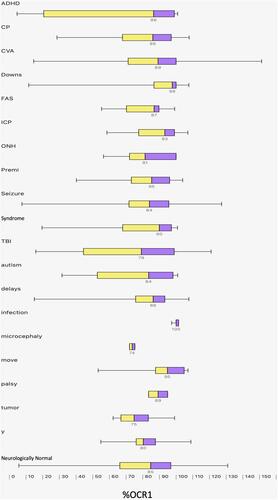
Figure 12 Influence of decade of experience; Box (interquartile range with median in the middle and whisker (95 percentile range) of %OCR in the Alaska OCR study from first decade starting in 1992, second decade and almost full third decade.
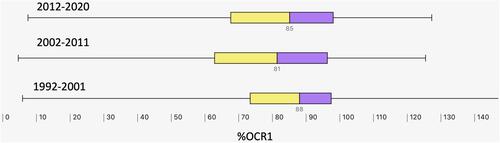
Table 1 Influence of Various Neurologic Conditions on Oculocardiac Reflex (Percent of Stable Baseline Heart Rate) Elicited by 10-Second, 200 Gram Square Wave Tension with No Anticholinergic Medication
Table 2 Influence of Anesthesiologists. The Eleven Main Anesthesiologists with More Than 60 Original Cases on Oculocardiac Reflex (Percent of Stable Baseline Heart Rate) Elicited by 10-Second, 200 Gram Square Wave Tension with No Anticholinergic Medication
Figure 13 Influence of anesthesiologist. During the Alaska OCR study, the median, interquartile range (box) and 95 percentile range (whiskers) for %OCR for the eleven anesthesiologists (Doc 1 through Doctor 11) and all others (other anesthesia) who provided the most prolific coverage general anesthesia during planned, outpatient strabismus surgery showing their number of cases (n = 69–212).
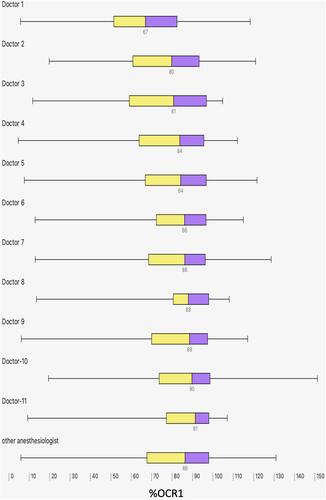
Figure 14 Influence of weight and age on %OCR. There was a significant trend toward less %OCR (no anticholinergic) for older and heavier patients during the Alaska OCR study. Multivariable regression found the correlation to be more robust for age than weight.
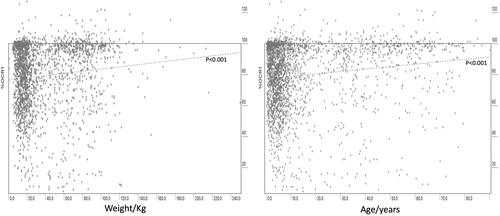
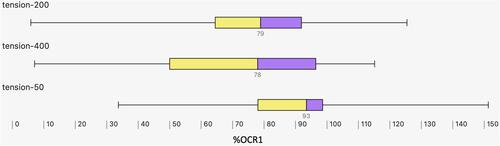
Figure 15 Impact of EOM Tension on %OCR. The Alaska OCR study predominantly performs uniform 200 gram, 10-second square wave tension on a carefully isolated extraocular rectus muscle (EOM). The median, the interquartile range (box) and 95 percentile (whiskers) for %OCR elicited by 400 gram tension was similar to 200 gram tension, but significantly more than the minimal %OCR elicited by very gentle, 50-gram EOM tension.