
Figures & data
Table 1 Patient Demographics
Figure 1 Surgical implantation of hook-shaped haptics into the sclera. (A) A previously reported method. The hook haptics have been implanted in the opposite direction of haptic withdrawal. (B) The improved method. The entire hook-shaped haptics have been buried in the direction in which they were pulled out. Arrow: the direction of implantation of hook haptics; dashed green line: the shape of scleral pocket; dashed blue line; IOL haptic inside the eye; solid blue line: IOL haptic; and solid black line: scleral wound.
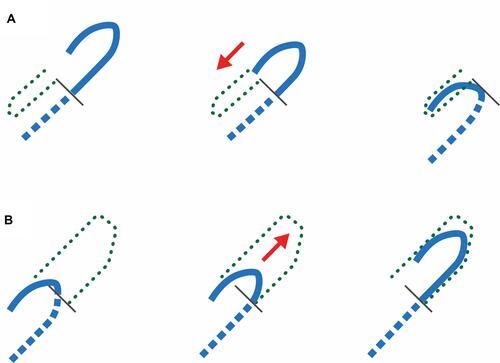
Figure 2 Modified intrascleral intraocular lens fixation surgery using a hook-shaped haptic intraocular lens. A scleral wound is created 180° and 1.5 mm away from the corneal limbus, using the knife attached to the 25G trocar (A and B). A scleral tunnel is created with the 23G knife (C and D). The intraocular lens is loaded into the cartridge (E) and inserted through the corneal incision (F). Two forceps are used (G and H) to grasp the trailing haptic and externalize it out of the eye (I). The other haptic is similarly grasped with the forceps (J) and externalized out of the eye (K). The hook-shaped part of the haptic is buried into the scleral tunnel (L and M). Following trocar removal, the wound closure is confirmed, and the surgery is completed (N).
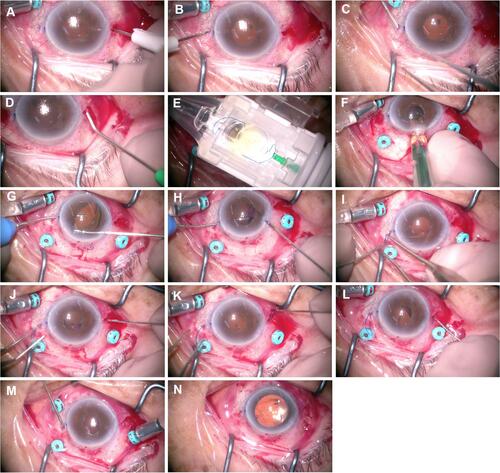
Table 2 Preoperative and 3-Month Postoperative Visual Acuity and Other Examination Values