
Figures & data
Figure 1 After limited conjunctival peritomy (A) 2 diagonally opposite scleral tunnels are fashioned and opened to the vitreous cavity by sclerotomy (B). A superior sclero-corneal incision is made (C). A bent hypodermic needle (D) receives the leading haptic in the anterior chamber (E) and the externalized haptic is sleeved by a silicone element for haptic stabilisation. The externalised (F) haptics are held at a measured distance from the tip with forceps and pocketed into the scleral tunnel (G) to bend the tip. Lens centration ensured at the end of the procedure (H).
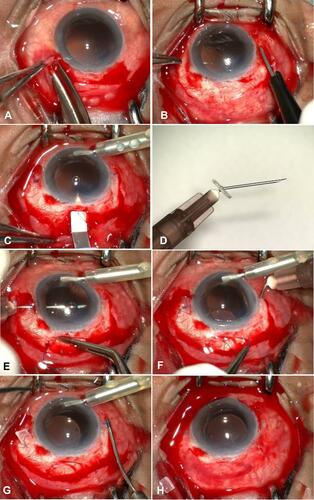
Table 1 Postoperative Complications (D – Day; W – Week; M – Months)
Figure 2 The uncorrected visual acuity (UCVA) trend (logMAR) shows a gradual improvement in vision over 6-week period mostly attributed to vitreous hemorrhage.
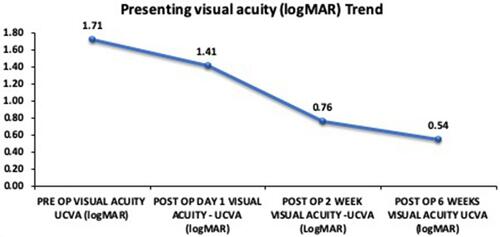
Figure 3 Lens deposits: Slit lamp capture on retro illumination shows cellular deposits on the surface of a scleral fixated intraocular lens 2wks post-surgery. Aphakia was caused by an open globe injury.
