Figures & data
Figure 1 Noninvasive meibography.
Notes: Photographs demonstrate the (A) meibography system and the (B) right upper eyelid and (C) right lower eyelid in a normal subject.
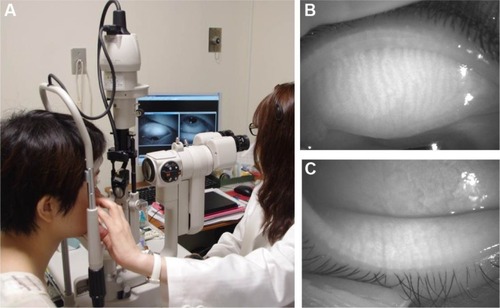
Table 1 Characteristics of the study subjects
Figure 2 Case 1: a 32-year-old woman with chalazion.
Notes: (A) Photograph of the tarsal conjunctiva of the left upper eyelid. Conjunctival injection and swelling at the nasal and lateral aspects were apparent. (B) Noninvasive meibographic image of the tarsal conjunctiva of the left upper eyelid and (C) its schematic representation. Meibomian glands in the central area of the eyelid had a normal appearance (arrows), whereas lesions at the nasal and lateral sides showed a lower reflectivity (open arrowheads) but contained small regions of higher reflectivity (closed arrowheads). (D) Photograph of the curettage specimen at the nasal side. (E) Noninvasive meibographic image of the curettage specimen and (F) its schematic representation. Low reflectivity was apparent for the granuloma lesion (open arrowhead) and high reflectivity for fatty granules (closed arrowheads). (G) Histopathologic analysis of the granuloma lesion. Fatty vacuoles surrounded by epithelioid cells, giant cells (arrowheads), and inflammatory cells were observed (hematoxylin–eosin; bar =100 μm).
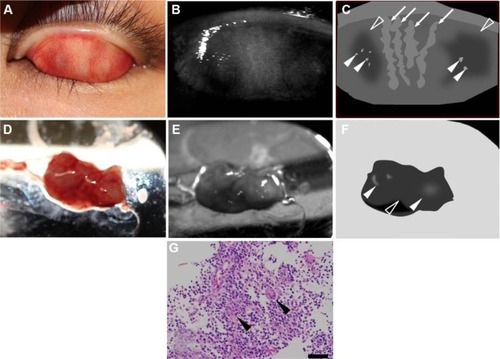
Figure 3 Case 5: a 61-year-old man with chalazion.
Notes: (A) Photograph of the tarsal conjunctiva of the right upper eyelid. A subconjunctival mass was observed at the nasal side. (B) Noninvasive meibographic image of the tarsal conjunctiva of the right upper eyelid and (C) its schematic representation. The mass showed overall low reflectivity (open arrowhead) but contained a central region of high reflectivity (closed arrowhead). (D) Photograph of the curettage specimen including fatty granules. (E) Noninvasive meibographic image of the curettage specimen and (F) its schematic representation. Noninvasive meibography detected overall low reflectivity of the granuloma lesion (open arrowhead) but high reflectivity of fatty granules (closed arrowheads). (G) Histopathologic analysis of the granuloma lesion. Inflammatory cells and dense fatty vacuoles were observed (hematoxylin–eosin; bar =100 μm).
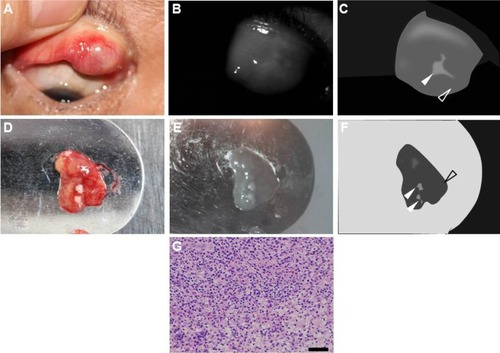
Figure 4 Case 6: an 87-year-old man with sebaceous carcinoma.
Notes: (A) Photograph of the left upper eyelid, revealing a yellow round mass without any defects in eyelashes. The longest dimension of the mass at the eyelid margin was 6 mm. There was no obvious change at the tarsal conjunctiva. (B) Noninvasive meibographic image of the tarsal conjunctiva of the left upper eyelid and (C) its schematic representation. Noninvasive meibography detected a poorly bordered mass lesion with relatively high reflectivity (closed arrowhead), a surrounding region of lower reflectivity (open arrowhead), and sharply marginated granules with high reflectivity (arrows). The dashed line and solid line indicate section lines for pathological observation (see below for further details). (D) Pathological section from the nasal side of the resected specimen. The section line is the dashed line in . The conjunctival (asterisk) and marginal (double asterisk) sides of the eyelid are indicated. No neoplastic cells were evident on the nasal side of the surgical margin, but a normal meibomian gland was apparent (hematoxylin–eosin; bar =1 mm). Pathological section from the central region of the tumor shown at (E) lower and (F) higher magnification. The section line is the solid line in . The conjunctival (asterisk) and marginal (double asterisk) sides of the eyelid are indicated. An ill-defined tumor lesion was observed at the eyelid margin (hematoxylin–eosin; bar =1 mm). The lesion contained small islands of tumor cells with fatty vacuoles. The tumor cells also manifested marked atypia with large and pleomorphic nuclei as well as many mitotic figures (closed arrowheads). Nucleoli were prominent and abnormal mitoses (open arrowhead) were often found (hematoxylin–eosin; bar =50 μm).
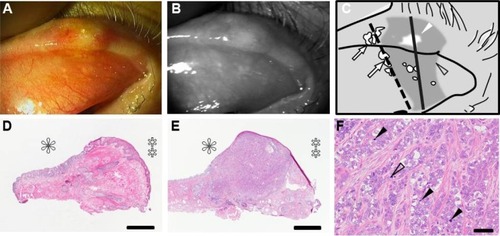
Figure 5 Case 7: an 89-year-old woman with sebaceous carcinoma.
Notes: (A) Photograph of the left upper eyelid. A red round mass with a diameter of 11 mm was observed. The nasal conjunctiva manifested injection. (B) Noninvasive meibographic image of the tarsal conjunctiva of the left upper eyelid and (C) its schematic representation. Noninvasive meibography detected a poorly bordered mass lesion with relatively high reflectivity (arrowheads) and a surrounding region of lower reflectivity. The dashed line and solid line indicate section lines for pathological observation (see below for further details). (D) Histopathologic section from the nasal side of the primary resected specimen. The section line is the dashed line in . The conjunctival (asterisk) and marginal (double asterisk) sides of the eyelid are indicated. Neoplastic cells were detected in both the eyelid margin (arrow) and conjunctiva on the nasal side (arrowhead) of the surgical margin (hematoxylin–eosin; bar =1 mm). Histopathologic section from the central region of the tumor shown at (E) lower and (F) higher magnification. The section line is the solid line in . The conjunctival (asterisk) and marginal (double asterisk) sides of the eyelid are indicated. An ill-defined tumor lesion was observed at the eyelid margin (hematoxylin–eosin; bar =1 mm). The lesion contained small islands of tumor cells with fatty vacuoles. The tumor cells also manifested marked atypia with large and pleomorphic nuclei as well as many mitotic figures (closed arrowheads). Nucleoli were prominent and abnormal mitoses (open arrowhead) were often found (hematoxylin–eosin; bar =50 μm).
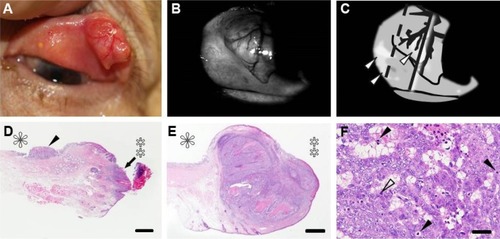
Figure 6 Case 8: an 82-year-old woman with recurrent sebaceous carcinoma.
Notes: (A) Photograph of the left upper eyelid. A nodular lesion with an irregular edge was detected. (B) Noninvasive meibographic image of the tarsal conjunctiva of the left upper eyelid and (C) its schematic representation. Noninvasive meibography revealed a poorly bordered lesion with relatively high intensity in both the nodular region and tarsal conjunctiva (arrowheads). The nodular region of the incisional biopsy is indicated (asterisk). Histopathologic analysis of the incisional specimen from the nodular lesion shown at (D) lower and (E) higher magnification. The nodular region was invaded by tumor (hematoxylin–eosin; bar =1 mm). (E) Neoplastic cells with fatty vacuoles were sparsely distributed in the specimen (hematoxylin–eosin; bar =50 μm).
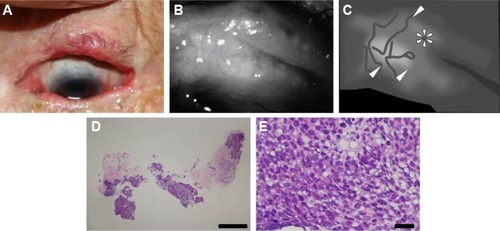
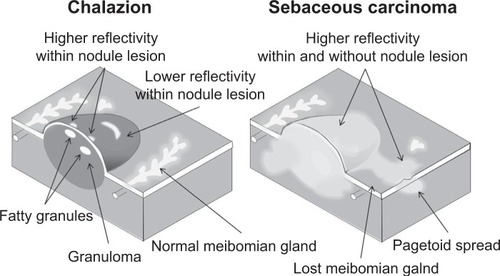
Figure 7 Schematic representation of the relationship between pathological characteristics and noninvasive meibography findings for chalazion and sebaceous carcinoma of the eyelid.
Notes: Chalazion is characterized by lipogranulomatous inflammation and liberated lipid granules within a connective tissue pseudocapsule. The granuloma appears as a lesion of low reflectivity in noninvasive meibographic images, whereas the fatty granules are visualized as sharply bordered structures of high reflectivity within the nodule lesion. Sebaceous carcinoma with its lipid content shows high reflectivity within the nodule lesion by noninvasive meibography. Tumor invasion into the surrounding tissue is also apparent as a poorly marginated irregular-shaped region of high reflectivity.