Figures & data
Figure 1 Pipkin classification of femoral head fractures. Type I: Fracture below fovea, Type II: Fracture above fovea, Type III: Type I or II with an associated femoral neck fracture, and Type IV: Type I or II with associated acetabular fracture.
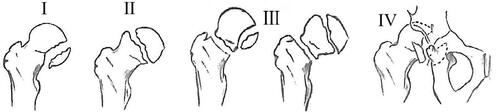
Figure 2 Demonstration of the suggested approaches for the management. (A) Medial approach to the hip. (B) Anterior, anterolateral, lateral, and posterior approaches. (C) Hip arthroscopy. (D) Surgical hip dislocation (SHD).
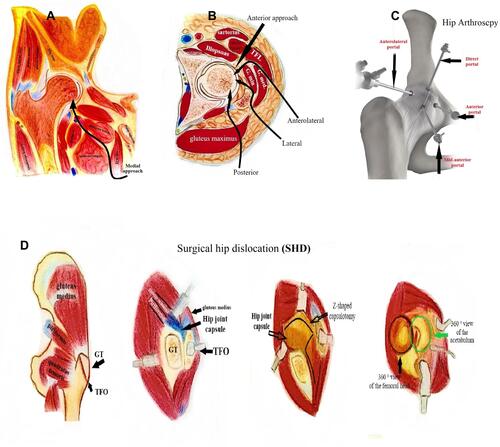
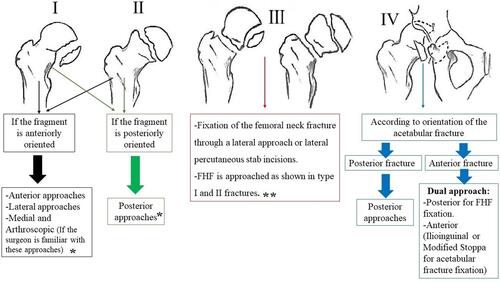
Figure 3 Example flow chart showing how to select the most appropriate approach for femoral head fractures (FHFs) surgical management as per Pipkin classification (Type I: Fracture below fovea, Type II: Fracture above fovea, Type III: Type I or II with an associated femoral neck fracture, and Type IV: Type I or II with associated acetabular fracture). * The mentioned approaches could be used for either fragment fixation or excision, ** better to avoid a posterior approach to preserve the blood supply.