Figures & data
Figure 1 Pre- and postoperative MRI and histopathological diagnosis for patient 1.
Notes: (A and B) Preoperative T2-weighted sagittal and T1 contrast-enhanced axial images showed a space occupying lesion with T2 heterogeneous hyperintensity and central dotty enhancement in the right parietal lobe. (C) Postoperative histopathological section (HE staining, magnification ×400) showed features of anaplastic astrocytoma (WHO grade III) with increased cellularity, nuclear atypia and mitotic activity. (D) T1 contrast-enhanced axial image at 3 months after operation showed an irregular mass with gross enhancement in the right basal ganglia and temporal lobe.
Abbreviations: MRI, magnetic resonance imaging; HE, hematoxylin–eosin; WHO, World Health Organization.
Abbreviations: MRI, magnetic resonance imaging; HE, hematoxylin–eosin; WHO, World Health Organization.
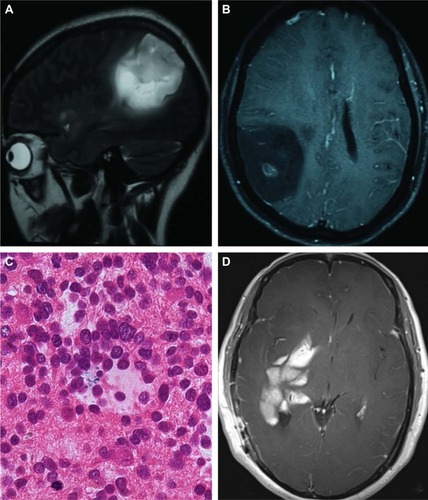
Figure 2 MRI during the second relapse for patient 1.
Notes: T1 contrast-enhanced axial images showed multiple oval and patchy nonhomogeneous enhancement lesions in the left cerebellar hemisphere (A) and parietal lobe (B).
Abbreviation: MRI, magnetic resonance imaging.
Abbreviation: MRI, magnetic resonance imaging.
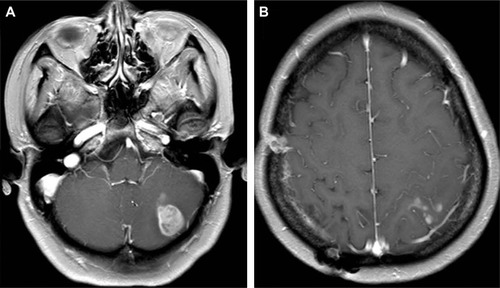
Figure 3 MRI comparison between pre- and post-apatinib for patient 1.
Notes: Before oral apatinib, FLAIR axial (A and B) and T1 contrast-enhanced axial images (C and D) showed multiple masses or nodular lesions with heterogeneous intensity and nonhomogeneous enhancement accompanied with central necrosis and peripheral edema in the left cerebellar hemisphere, parieto-frontal lobes. After 6 weeks medication with apatinib, FLAIR axial (E and F) and T1 contrast-enhanced axial images (G and H) showed all the lesions and peripheral edema significantly reduced compared with pre-apatinib MRI.
Abbreviations: FLAIR, fluid attenuation inversion recovery; MRI, magnetic resonance imaging.
Abbreviations: FLAIR, fluid attenuation inversion recovery; MRI, magnetic resonance imaging.
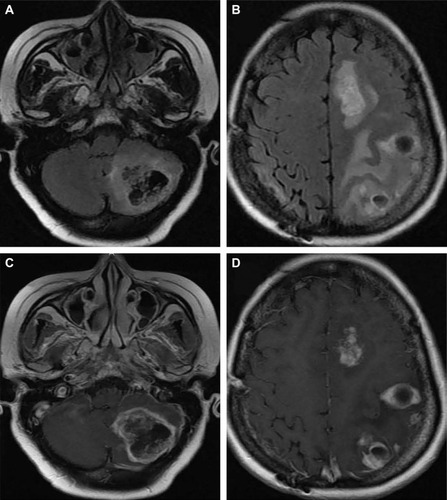
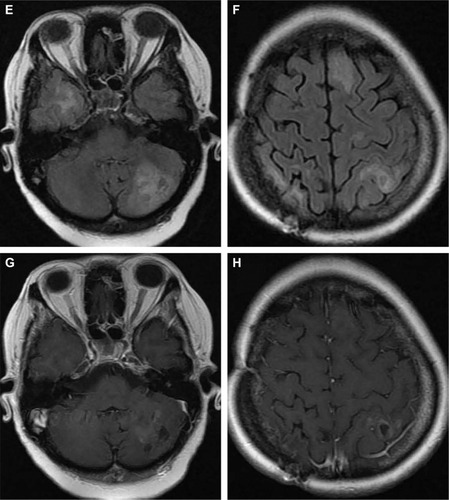
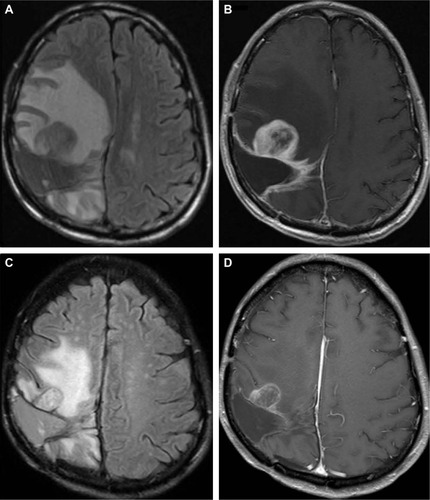
Figure 4 Pre- and postoperative MRI between the first and second operation and histopathological diagnosis for patient 2.
Notes: (A) T1 contrast-enhanced axial image showed an irregular occupying mass with nonhomogeneous enhancement accompanied with necrosis and peripheral edema at the right parieto-occipital lobes before the first operation. (B) Histopathological section (HE staining, magnification ×200) after surgery showed the features of glioblastoma multiforme (WHO grade IV), with highly increased cellularity, marked nuclear atypia and mitotic activity, hemorrhage and pseudopalisading necrosis. (C) At 6 months after the first operation, T1 contrast-enhanced axial image showed that a mass with nonhomogeneous enhancement reappeared at the primary location, accompanied with central necrosis and peripheral edema. (D) At 43 days after the second operation, T1 contrast-enhanced axial image showed a recurrent nodular enhanced lesion in the front edge of the operative cavity accompanied with obvious peripheral edema.
Abbreviations: MRI, magnetic resonance imaging; HE, hematoxylin–eosin; WHO, World Health Organization.
Abbreviations: MRI, magnetic resonance imaging; HE, hematoxylin–eosin; WHO, World Health Organization.
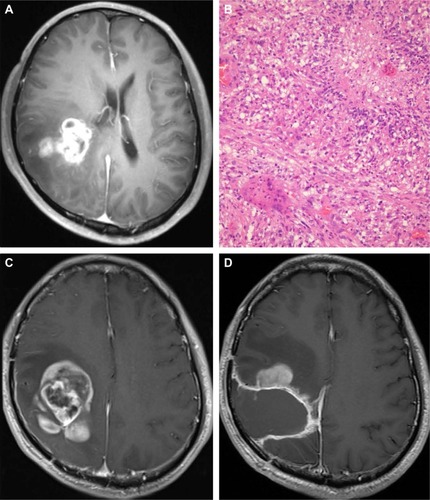
Figure 5 MRI comparison between pre- and post-apatinib for patient 2.
Notes: Before oral apatinib, FLAIR axial (A) and T1 contrast-enhanced axial images (B) showed an enlarged recurrent lesion accompanied with central necrosis and obvious peripheral edema. At 4 weeks medication of apatinib, FLAIR axial (C) and T1 contrast-enhanced axial images (D) showed that the lesion and peripheral edema were significantly reduced compared with pre-apatinib MRI.
Abbreviations: MRI, magnetic resonance imaging; FLAIR, fluid attenuated inversion recovery.
Abbreviations: MRI, magnetic resonance imaging; FLAIR, fluid attenuated inversion recovery.