Figures & data
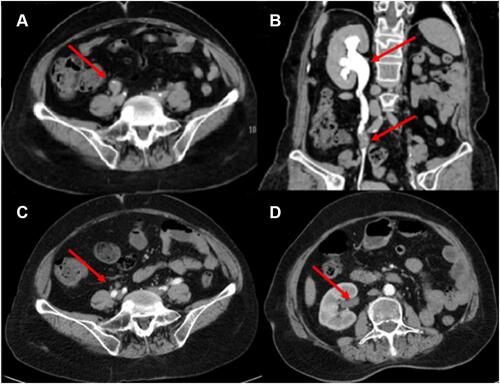
Figure 1 Abdomen enhancement CT scan and pathology of surgical specimen (A–D). (A) CT images showed the filling defects in the upper middle segment of the left ureter (red arrow), suggesting ureteral carcinoma. (B) 100x magnification image of the UTUC. The cancer cells were papillary, nested, densely arranged in sheets, with large and deeply stained nuclei (red arrow). H&E stained. (C) Immunohistochemistry of PD-L1 expression in the tumor tissue (DAKO 22C3). PD-L1 antibody exhibited CPS ≥10 at 10× magnification. (D) PD-L1 antibody exhibited CPS ≥ 10 at 20× magnification.
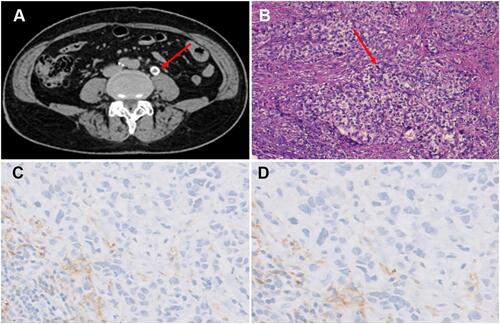
Figure 2 Abdomen CT scans after 6 months chemotherapy with cisplatin and gemcitabine (A and B) and after 6 cycles of immunotherapy with pembrolizumab (C and D), images on the same sections. (A) Compared with , the patient’s left abdominal aortic lymphadenopathy was enlarged (red arrow). (B) The left main adrenal gland and medial branch nodules were thickened (red arrow), suggesting that the tumor has metastasized. (C) Abdominal aortic lymph node enlargement shrank significantly (red arrow). (D) The left main adrenal nodule disappeared (red arrow), indicating the stabilization of disease progression.
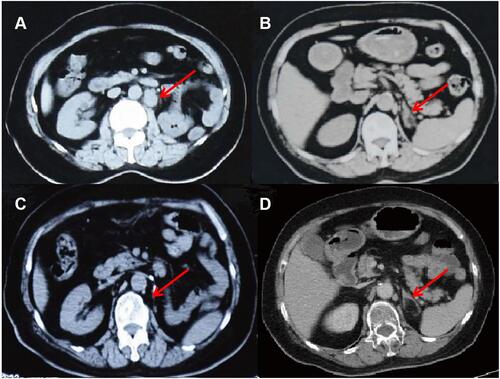
Table 1 Clinical Relevant Somatic Mutation Identified in Present Case of UTUC
Figure 3 CT urogram. (A) Tumor recurrence in the middle right ureter (red arrow). (B) As a result of blockage in the middle ureter, the right hydronephrosis expanded (red arrow). (C) After 3 cycles of a combination of pembrolizumab and erdafitinib, the thickening of the wall of the right middle ureter was significantly reduced (red arrow). (D) The expansion of the right renal pelvis and the effusion were obviously disappeared (red arrow).