Figures & data
Figure 1 Chest CT scan of February 19, 2019 representing a left upper lobe pulmonary nodule of 12.4 mm in lung window (A) and a prevascular adenopathy in mediastinal window of 12.7 mm (B). Chest X-Ray with the cross-sectional height at which pulmonary nodule is located (C).
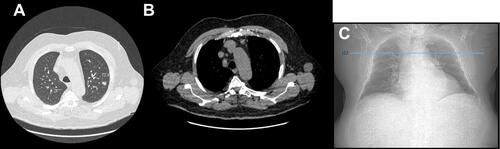
Figure 2 Pre-therapeutic TEP scan of March 19, 2019 representing a hypermetabolism of the left upper lobe pulmonary nodule (SUVmax: 3.29) (A and B); and an intense hypermetabolism focus in the left interlobular lymph node (SUVmax: 5.55) (C).
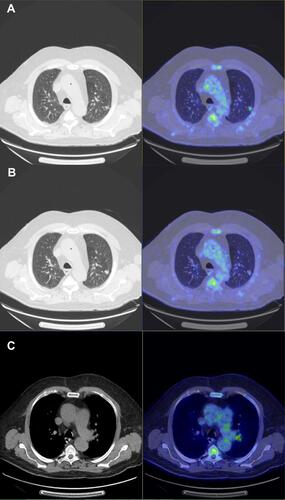
Figure 3 CT scan of February 5, 2020 revealing a mediastinal lymph node progression (RECIST 1.1) with a 21 mm adenopathy in front of the aortic arch and a second one of 18 mm in the pretracheal space.
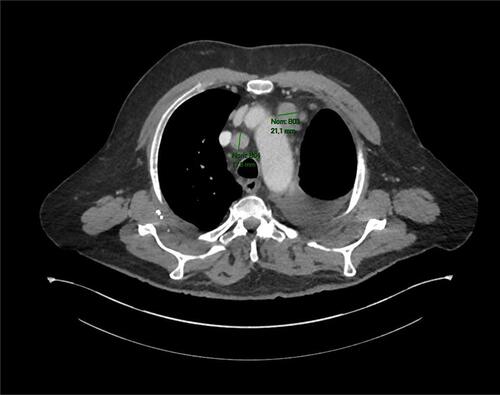
Figure 4 CT scan of June 11, 2020 showing a partial response aspect (RECIST 1.1) of two mediastinal lymph node involvements, the first in front of the aortic arch (A) and a second one of 18 mm in the pretracheal space (B).
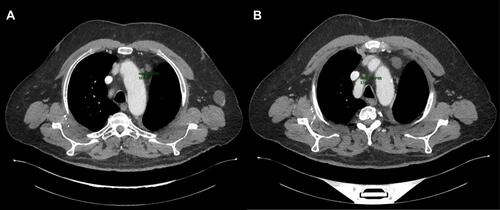
Figure 5 CT scan of December 28, 2020 representing a lymph node and pleural progression.

Figure 6 Schematic representation of a part of MET gene, including exon 14, its splicing site, and the site of the mutation.
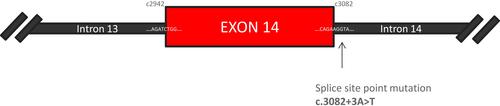
Figure 7 MET structure, consists of several domains. The extracellular part is composed by SEMA domain shared between the two chains, a PSI domain, and four IPT domains. The intracellular part is composed by the juxtamembrane domain encoded by exon 14, the kinase domain, and the multisubstrate docking site.
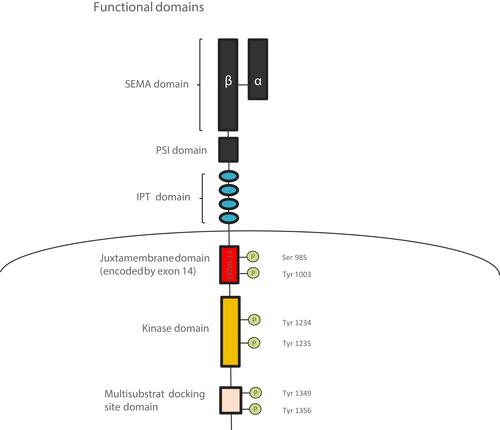
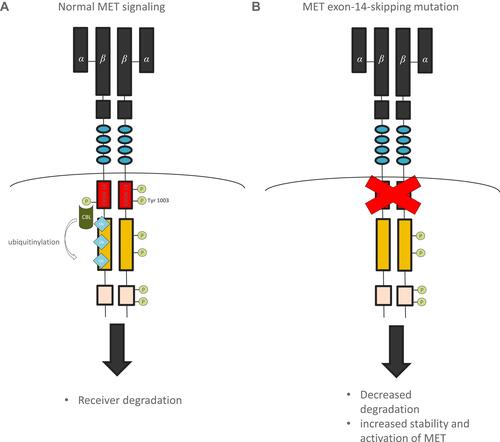
Figure 8 Mechanism of MET signaling regulation. Normal MET signaling (A) and abnormal signaling with MET-exon-14 skipping mutation (B).