Figures & data
Figure 1 (A) Baseline axial CT performed 360 min after the symptom onset showing a faint hypodensity in the left frontotemporoparietal lobe with a RAPID-ASPECTS of score 1. (B) CTA showed a complete occlusion of the left M1. (C) The RAPID-CTP analysis demonstrated a complete infarct volume of 76 milliliters (mL), entailing a small infarcted core within a large volume of penumbra in the right internal carotid artery vascular territory. The configured Tmax > 6-second volume representing the combination of the infarcted core volume and hypoperfused brain was 143 mL in the left cerebral hemisphere, deriving a mismatch ratio of 1.9.
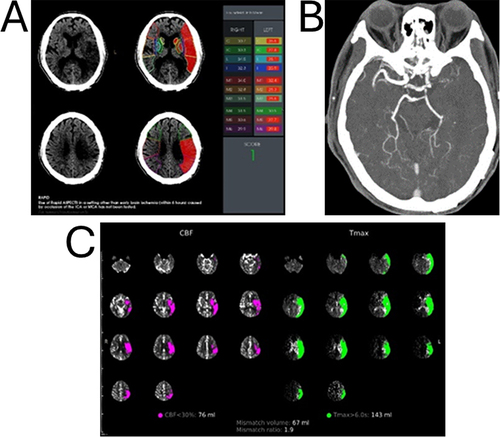
Figure 2 (A) Digital subtraction angiography (DSA), left internal carotid artery injection, anteroposterior (AP) view, showing proximal left middle cerebral artery (MCA) M1 occlusion with intraluminal filling defect due to thrombosis. (B) DSA, AP view, showing a 4-mm × 40-mm Solitaire X (Medtronic) stent-retriever (SR) un-sheathed in the affected MCA with reopening of the vessel. (C) DSA, AP view, post-thrombectomy, showing successful recanalization and restoration of blood flow.
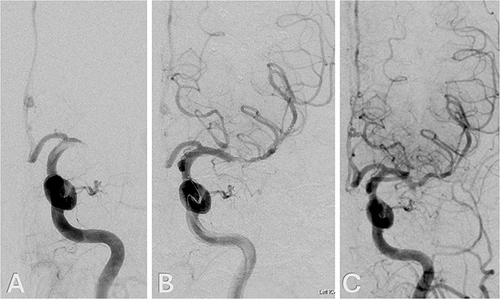
Figure 3 (A) Photograph showing a reddish brown gelatinous thrombus extracted by the stent-retriever. Panels B and C. Photomicrographs of the retrieved thrombi, Hematoxylin and eosin stain, x 100 (B) and x 400 (C), showing fibrin and blood admixed with metastatic adenocarcinoma, which is composed of tubular or fused glands, with pseudostratified epithelium, consistent with colorectal origin. Immunohistochemical stains showed CK7-negative, CD20-positive, and CDX-2-positive.
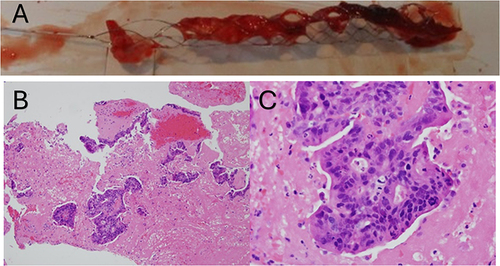
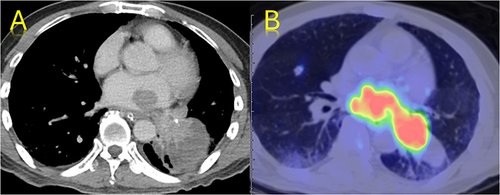
Figure 4 (A) Contrast-enhanced axial CT and (B) PET/CT fusion images of the thorax showing a left lung mass invading the left atrium and pulmonary vein.