
Figures & data
Figure 1 Histological examination with immunohistochemistry and hematoxylin-eosin staining (e/e).
Notes: (A) e/e 20× magnification; (B) chromogranin 20× magnification; (C) Synaptophysin 20× magnification; (D) Ki-67 40× magnification.
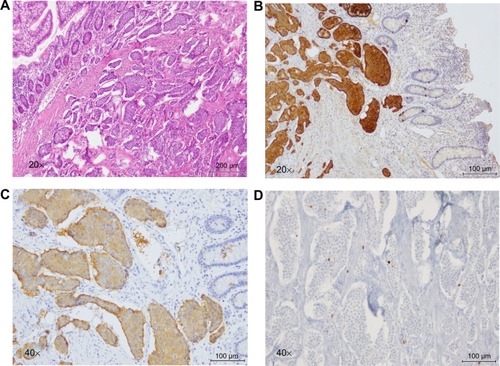
Figure 2 Liver metastatic NET.
Notes: (A and B) Contrast-enhanced CT. (A) A double-contrast study of the stomach; the difference between the abdominal parenchyma visualized in the two examinations lies in the different degrees of filling of the stomach and in the patient’s different breaths. Before treatment, the hepatic lesion of the fourth segment shows inhomogeneous enhancement (yellow arrow). (B) After treatment, the lesion’s size and density remain stable (yellow arrow). This is SD according to both the RECIST and CHOI criteria.
Abbreviations: LVR, liver; RPV, right branch of the portal vein; ST, stomach; LKD, left kidney; SPL, spleen; NET, neuroendocrine tumor; CT, computed tomography; SD, stable disease.
Abbreviations: LVR, liver; RPV, right branch of the portal vein; ST, stomach; LKD, left kidney; SPL, spleen; NET, neuroendocrine tumor; CT, computed tomography; SD, stable disease.
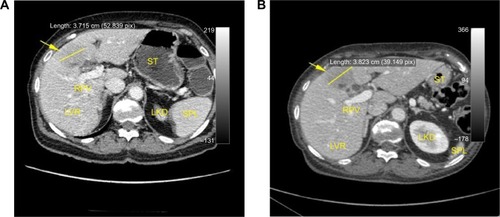
Figure 3 Liver metastatic NET.
Notes: (A–D) Contrast-enhanced CT. (A and C) Double-contrast study of the stomach. The difference between the abdominal parenchyma visualized in the two examinations lies in the different degree of filling of the stomach and in the patient’s different breaths. Before treatment, the hepatic lesions of the seventh and eighth segments appear as soft hypodense inhomogeneous lesions (yellow arrow). (B and D) After treatment, the lesions are not more appreciable.
Abbreviations: LVR, liver; ST, stomach; SPL, spleen; LKD, left kidney; NET, neuroendocrine tumor; CT, computed tomography.
Abbreviations: LVR, liver; ST, stomach; SPL, spleen; LKD, left kidney; NET, neuroendocrine tumor; CT, computed tomography.
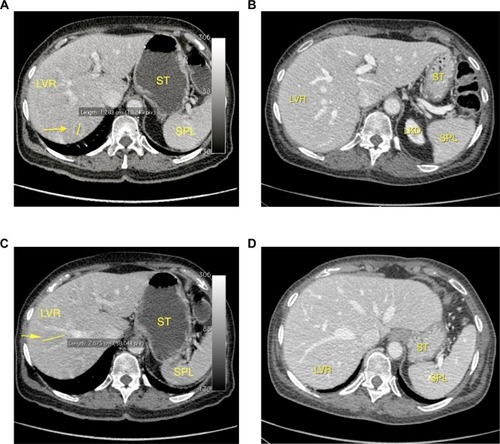
Table 1 After 3 months of OCT LAR 30 mg, an almost complete clinical response was observed in the patient, with symptom regression and PS recovery from ECOG PS 2 to ECOG PS 0