Figures & data
Figure 1 Functionalist model explaining the realization of action.
Notes: This model can be applied to all our actions, eg, increasing the dose of insulin if blood glucose is high. The desire–belief pair represents the main pro-attitude causing this action, playing an instrumental role; eg, the desire to avoid the recurrence of hyperglycemia and the belief that increasing the insulin dose will satisfy this desire. In addition, the patient must have knowledge (eg, that insulin lowers blood glucose) and skills (knowing how to decide on the insulin dose). Emotions also influence desires, such as fear of weight gain, which may reduce the desire to avoid hyperglycemia. Furthermore, other beliefs may also alter this desire, such as the belief that increasing the insulin dose will result in the risk of hypoglycemia. Thus, beliefs, in addition to the instrumental role that makes them the driver of our actions, can perform another role associated with emotions. These two types of mental states are triggered by events (for example, the recent occurrence of hypoglycemia). In addition, in this figure, we have represented the possible effect of feelings (such as pain and pleasure) and the involvement of exogenous factors as resources necessary for the realization of the action. This “physiology of the mind” is described in detail in the cited reference. Reach G. The Mental Mechanisms of Patient Adherence to Long Term Therapies: Mind and Care, Foreword by Pascal Engel, Philosophy and Medicine Series, Springer, 2015. This figure was adapted from a figure published in The Mental Mechanisms of Patient Adherence to Long-Term Therapies, Mind and Care, by Gérard Reach Springer © 2015, with Springer’s permission for reprint.Citation15
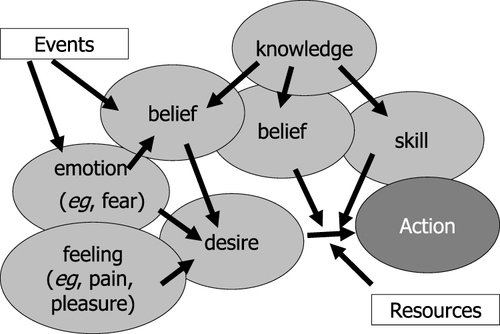
Figure 2 Involvement of heuristics and emotions in patient non-adherence.
Notes: Explanatory model of the tendency to inaction (lack of adjustment of the insulin dose, and more generally hesitation to initiate treatment): role of uncertainty making the decision difficult and lack of time, leading to the use of heuristics and thus to an overestimation of the risk of unfortunate events, and implication of emotions and aversion to losses. Reprinted from Diabetes Metab, volume 39, Reach G. A psychophysical account of patient non-adherence to medical prescriptions. The case of insulin dose adjustment. 50–55, Copyright (2013), with permission from Société Francophone du Diabète, published by Elsevier Masson SAS. All rights reserved.Citation90
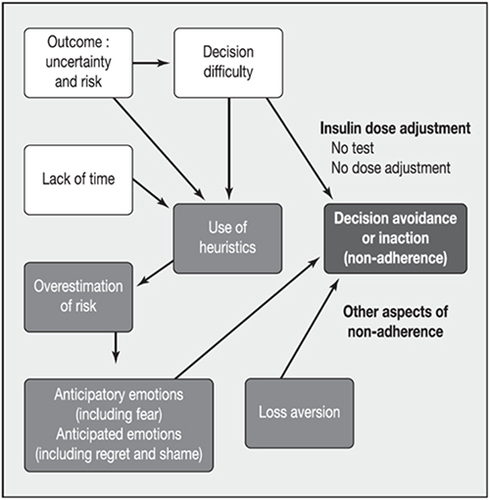
Figure 3 Intentionality and adherence.
Notes: Both non-adherence and adherence can be intentional or non-intentional. An episode of unintentional non-adherence may lead to intentional non-adherence, if the patient observes the absence of untoward consequences (arrow 1). Adherence may initially be intentional to give way to unintentional adherence through habit (arrow 2).
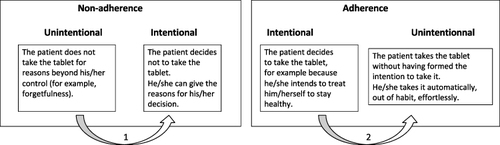
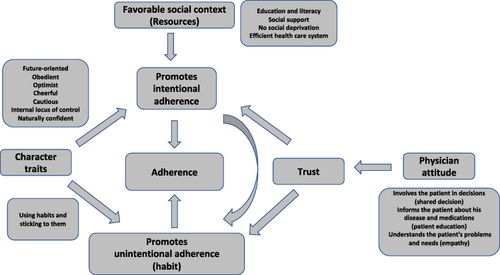
Figure 4 Integrated mechanistic model of adherence: how is patient adherence possible?.
Notes: The model shows that there are two gateways to adherence: promoting both intentional and unintentional adherence. Trust, generated by a positive physician’s attitude, plays a central role in linking patient and physician-related determinants. The vertical curved arrow linking intentional and unintentional adherence suggests that in the first step, one has to make an effort to be adherent and that this effort can gradually give way to the force of habit.