Figures & data
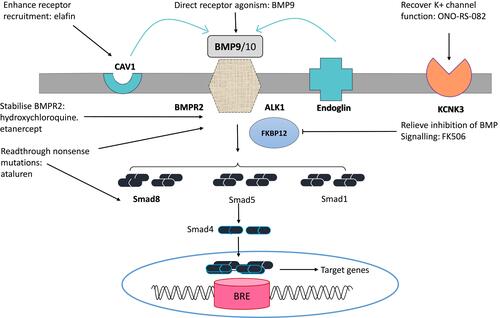
Figure 1 Typical histopathological characteristics of PAH.Notes: (A, B) Lung tissue from a HPAH patient with a mutation in the CAV1 gene (grades I and II). Hematoxylin and eosin staining may show pulmonary vascular smooth muscle cell proliferation, medial thickening of small pulmonary arteries (A, arrows), as confirmed by immunohistochemical staining of α‐smooth muscle actin (B, arrows).Citation117 (C, D) Lung biopsy from a HPAH patient with a mutation in the KCNK3 gene. (C) Fibrosis (arrowhead), intimal proliferation, and recanalization (asterisk), with an adjacent angiomatoid lesion (arrow) typical of HPAH/IPAH (grade III). (D) Grade IV PAH disease may include plexiform lesions characterized by intimal and endothelial proliferation (arrow).Citation118 Copyright ©2017. John Wiley and Sons. Reproduced from Ma L, Chung WK. The role of genetics in pulmonary arterial hypertension. J Pathol. 2017;241(2):273–280.Citation4
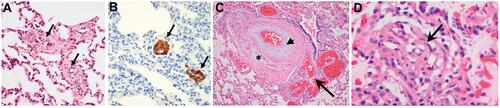
Figure 2 From genetics to pharmacological treatment.Notes: Bone morphogenetic protein receptor II, BMPR-II; BMP-responsive element, BRE; Caveolin-1, CAV1; 12-kDa FK506-binding protein, FKBP12. BMP-II signaling in pulmonary vascular endothelial cells may be mediated by the ligands BMP9 and BMP10 through the ALK1/BMPR2 receptor complex. Endoglin may serve as an accessory receptor. Pathway may be mediated via phosphorylation of the receptor Smads (Smad1, 5 and 8), which in turn may interact with Smad4 and translocate to the nucleus, modulating genes that contain BREs. CAV1 may promote receptor colocalization, while KCNK3 encodes a potassium channel that may enhance pulmonary vascular tone. Genes that are mutated in HPAH are in bold. Potential therapeutic strategies targeted to these signaling pathways may include: administration of BMP9 ligand, enhancing availability of functional BMPR2 receptors (hydroxychloroquine, etanercept), enhancing readthrough of nonsense mutations to restore functional BMPR2 or Smad8 protein (ataluren), promoting downstream signaling by relieving FKBP12 inhibition of BMP type 1 receptors (FK506), enhancing CAV1-mediated receptor recruitment (elafin), or recovering KCNK3 potassium-channel current (ONO-RS-082). Adapted with permission from Morrell NW, Aldred MA, Chung WK, et al. Genetics and genomics of pulmonary arterial hypertension. Eur Respir J. 2019;53(1):1801899.Citation107