Figures & data
Table 1 Characteristics of participants enrolled in the study
Figure 1 Tc17 cell frequency was significantly higher in patients with HBV-ACLF.
Notes: (A) Tc17 cells were analyzed by flow cytometry. In this study, Tc17 cells were defined as CD3+ CD8+ IL-17A+ cells. Gating strategy for the analysis of Tc17 cells was shown. (B) Representative dot plots of Tc17 cells from NC, patients with CHB, and patients with HBV-ACLF. The value in the upper right quadrant indicated the frequency of Tc17 cells. (C) Tc17 cells were significantly higher in patients with HBV-ACLF than in either patients with CHB (P=0.002) or NC subjects (P<0.001). Moreover, the frequency of Tc17 cells was significantly higher in cirrhotic patients with HBV-ACLF than in non-cirrhotic patients with HBV-ACLF (P=0.034). No differences were observed in Tc17 cells between HBeAg-positive and HBeAg-negative patients in the CHB group and in patients with HBV-ACLF. *P<0.05; **P<0.01; ***P<0.001.
Abbreviations: ACLF, acute-on-chronic liver failure; CHB, chronic hepatitis B; eAg-P, HBeAg-positive; FSC, forward scatter; eAg-N, HBeAg-negative; HBV, hepatitis B virus; ns, not significant; NC, normal control; SSC, side scatter; Tc17, IL-17-producing CD8+ T.
Abbreviations: ACLF, acute-on-chronic liver failure; CHB, chronic hepatitis B; eAg-P, HBeAg-positive; FSC, forward scatter; eAg-N, HBeAg-negative; HBV, hepatitis B virus; ns, not significant; NC, normal control; SSC, side scatter; Tc17, IL-17-producing CD8+ T.
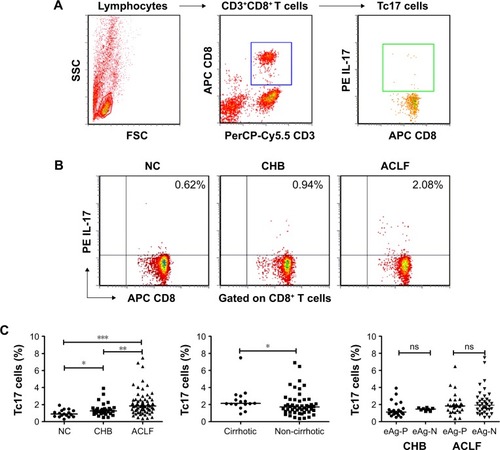
Figure 2 Tc17 cells may play a proinflammatory role in the pathogenesis of HBV-ACLF.
Notes: Tc17 cells were found to be associated with Tbil levels, PTA levels, AST levels, and ALB levels in patients with CHB (A) and patients with HBV-ACLF (B). The frequencies of Tc17 cells were significantly higher in non-surviving patients than in surviving patients (P<0.001). Moreover, the frequencies of Tc17 cells were positively correlated with MELD, MELD-Na, and CLIF-C ACLF scores (C). Lg (AST), AST levels were transformed into log10. Solid line, linear growth trend; r, correlation coefficient. ***P<0.001.
Abbreviations: ACLF, acute-on-chronic liver failure; AST, aspartate aminotransferase; ALB, albumin; CHB, chronic hepatitis B; CLIF-C, chronic liver failure consortium; HBV, hepatitis B virus; MELD, model for end-stage liver disease; PTA, prothrombin time activity; TB, total bilirubin; Tc17, IL-17-producing CD8+ T.
Abbreviations: ACLF, acute-on-chronic liver failure; AST, aspartate aminotransferase; ALB, albumin; CHB, chronic hepatitis B; CLIF-C, chronic liver failure consortium; HBV, hepatitis B virus; MELD, model for end-stage liver disease; PTA, prothrombin time activity; TB, total bilirubin; Tc17, IL-17-producing CD8+ T.
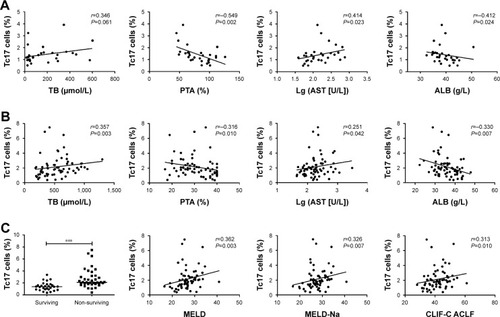
Figure 3 Increased Tc17 cell frequency at admission indicated poor prognosis in HBV-ACLF.
Notes: (A) The prognostic value of Tc17 cell frequency was assessed by the ROC curve analysis. The AUROC for Tc17 cell frequency was 0.826 (95% CI: 0.712–0.908, P<0.001). The Youden index was used to identify the optimal cutoff value. With a cutoff value of 1.6%, the sensitivity was 86.84% (95% CI: 71.9%–95.6%) and the specificity was 75% (95% CI: 55.1%–89.3%). Moreover, no significant differences were found between AUROC values obtained with Tc17 cell frequency and those obtained with the MELD (AUROC=0.769, P=0.437), MELD-Na (AUROC=0.782, P=0.552), or CLIF-C ACLF (AUROC=0.773, P=0.474) scores, indicating that Tc17 cell frequency at admission may have a prognostic value equivalent to that of these accepted prognostic scores. (B) Survival was evaluated using Kaplan–Meier curves, and the statistics were compared by log-rank tests. Significant differences were found between the higher group (Tc17 cell frequency >1.6%) and the lower group (Tc17 cell frequency ≤1.6%) in both 30-day (chi-square=8.545, P=0.0035) and 90-day (chi-square=23.98, P<0.0001) survival.
Abbreviations: AUC, area under curve; ACLF, acute-on-chronic liver failure; AUROC, area under the ROC curve; CLIF-C, chronic liver failure consortium; Cum, cumulative; HBV, hepatitis B virus; MELD, model for end-stage liver disease; ROC curve, receiver operating characteristic curve; Tc17, IL-17-producing CD8+ T.
Abbreviations: AUC, area under curve; ACLF, acute-on-chronic liver failure; AUROC, area under the ROC curve; CLIF-C, chronic liver failure consortium; Cum, cumulative; HBV, hepatitis B virus; MELD, model for end-stage liver disease; ROC curve, receiver operating characteristic curve; Tc17, IL-17-producing CD8+ T.
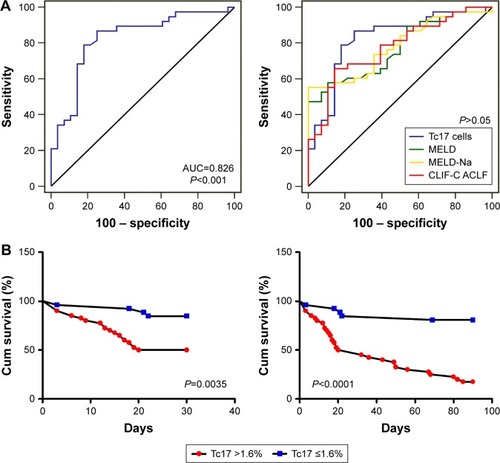
Table 2 Characteristics of patients with HBV-ACLF according to clinical outcome
Table 3 Factors associated with mortality in patients with HBV-ACLF by using the Cox regression analysis
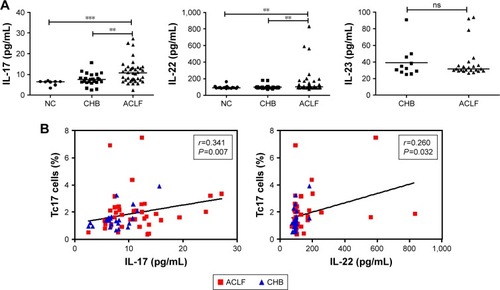
Figure 4 Tc17 cell frequency was positively correlated with serum IL-17A and IL-22 levels.
Notes: (A) Serum levels of cytokines (IL-17A, IL-22, and IL-23) were determined by a FlowCytomix assay. IL-17A levels and IL-22 levels were higher in patients with HBV-ACLF than in patients with CHB and NC subjects. However, the IL-23 level did not differ between patients with HBV-ACLF and those patients with CHB. (B) Positive correlations were found between the frequency of Tc17 cells and the levels of both IL-17A (r=0.341, P=0.007) and IL-22 (r=0.260, P=0.032). However, no correlation was found between Tc17 cell frequency and IL-23 level (r=0.030, P=0.867). These data indicated that Tc17 cells may be an additional source of IL-17 in HBV-infected patients. **P<0.01; ***P<0.001. Solid line, linear growth trend; r, correlation coefficient.
Abbreviations: ACLF, acute-on-chronic liver failure; CHB, chronic hepatitis B; HBV, hepatitis B virus; NC, normal control; ns, not significant; Tc17, IL-17-producing CD8+ T.
Abbreviations: ACLF, acute-on-chronic liver failure; CHB, chronic hepatitis B; HBV, hepatitis B virus; NC, normal control; ns, not significant; Tc17, IL-17-producing CD8+ T.