Figures & data
Figure 1 First-level approach to patients presenting with lymphoproliferation.
Notes: This algorithm identifies the patients with a clinical picture suggestive for infection (green boxes) and malignancy (red boxes) and those with a less defined clinical picture (yellow boxes). The diagnostic approach for patients with suspected infection or malignancy is provided, evidencing that first-level analysis and US imaging are mandatory in patients with high risk of malignancy. On the other hand, when infection is suspected, the choice about performing laboratory and imaging investigations relies on the individual situation. Patients without a clearly defined diagnosis should be periodically re-assesses and eventually undergo further investigations. *There is no uniform consensus regarding the need to perform prolonged antibiotic treatment in NTM lymphadenitis, and some authors suggest to perform only clinical observation. **PET and CT can be performed also before lymph nodal biopsy based on the clinical judgement.
Abbreviations: CMV, Cytomegalovirus; CRP, C-reactive protein; CT, Computed tomography; EBV, Epstein-Barr virus; ESR, Erythrocyte sedimentation rate; GAS, Group A Streptococcus, HLH, Hemophagocytic lymphohistiocytosis; IGRA, Interferon-gamma release assay; NTM, Nontuberculous mycobacteria; PET, Positron emission tomography; TST, tuberculin skin test; US, Ultrasound.
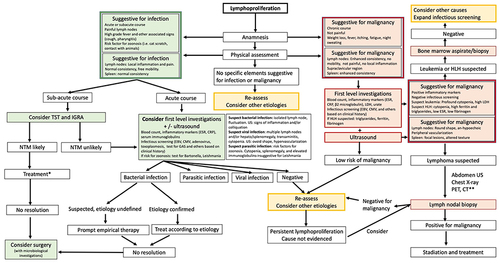
Figure 2 US findings in lymphadenopathies with different etiology.
Notes: (A) Reactive lymphadenopathy in a patients with acute respiratory infection. Lymph nodes are typically featured by ovoid shape, clear evidence cortical differentiation, and hilar vascularization; (B) Bacterial lymphadenitis, in which some areas of colliquation are evident; (C) Lymph nodes in a patient with Hodgkin lymphoma. Lymph nodes are featured by round shape, hypo-anechoic texture, absence of cortical differentiation, and scarce, peripheral vascularization; (D) Lymph nodes in a patient with immune dysregulation and granulomatous lymphadenitis. In this condition, lymph nodes can This show some overlapping features with malignancies, including round shape, hypoechoic texture, and irregular vascularization.
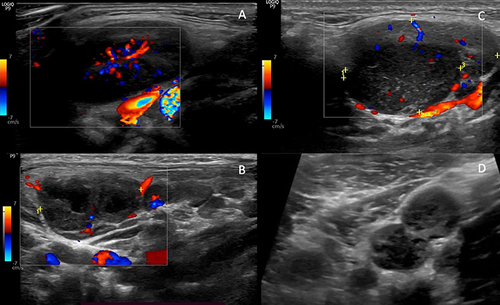
Figure 3 US findings in splenomegaly with different etiology.
Notes: (A) Splenomegaly in a patient with acute EBV infection, featured by a mildly disomogeneous texture and absence of focal lesions; (B) Focal spleen lesion in a patient with Bartonella henselae infection. In this condition, the lesions are usually multiple and anechoic, but during the disease evolution a peripheral hypoechoic are can be detected; (C) Splenomegaly in a patient with Gaucher disease, featured by homogeneous spleen texture (D) Spleen involvement in Hodgkin lymphoma, in which focal hypo-anechoic lesions are evident.
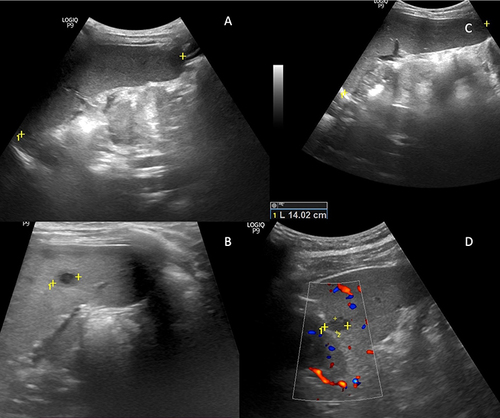
Table 1 Inborn Errors of Immunity Associated with Lymphoproliferation
Figure 4 Overlaps in the pathogenesis of lymphoproliferation in IEI, infections, and malignancies.
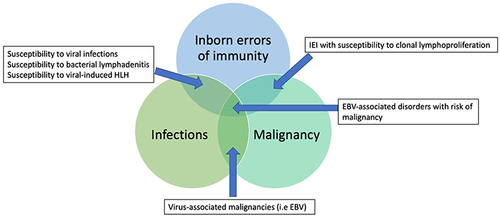
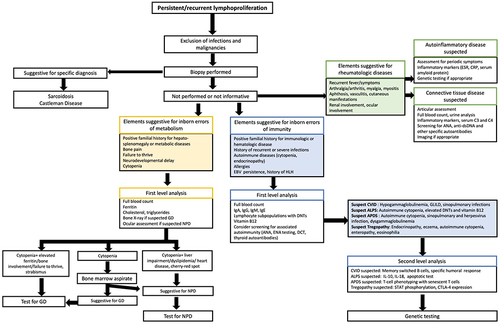
Figure 5 Diagnostic algorithm for the identification of rare causes of lymphoproliferation.
Notes: In patients with persistent/recurrent lymphoproliferation, when a diagnosis has not been reached, the search for signs associated with IEI (blue boxes), IEM (yellow boxes), and rheumatologic diseases (green boxes) could lead to appropriate investigations, and finally to the identification of rare etiologies underlying lymphoproliferation.
Abbreviations: APDS, activated phosphoinositide 3-kinase δ syndrome; ALPS, Autoimmune lymphoproliferative syndrome; ANA, Antinuclear antibodies; CVID, Common variable immunodeficiency; DCT, Direct Coombs test; EBV, Epstein-Barr virus; ENA, extractable nuclear antigen; GD, Gaucher disease; GLILD, Granulomatous lymphocytic interstitial lung disease; HLH, Hemophagocytic lymphohistiocytosis; IEI, Inborn errors of immunity, IEM, Inborn errors of metabolism; NPD, Niemann-Pick diseases.