Figures & data
Figure 1 Bisphosphonate structure, bone mineral binding, and biochemical mechanisms.
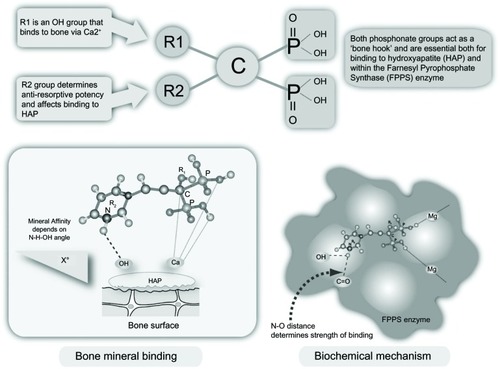
Figure 2 Inhibition of the mevalonate pathway by statins and bisphosphonates.
Abbreviation: HMG Co-A, 3-hydroxy-3-methylglutarylcoenzyme A.
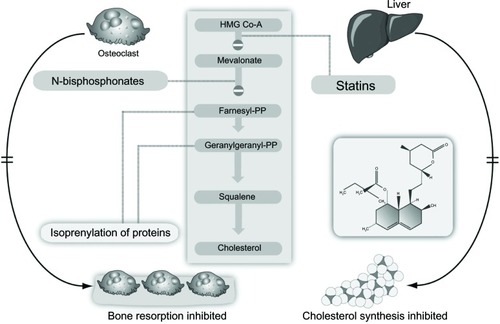
Figure 3 Paracellular, transcellular route, and tight junctions.
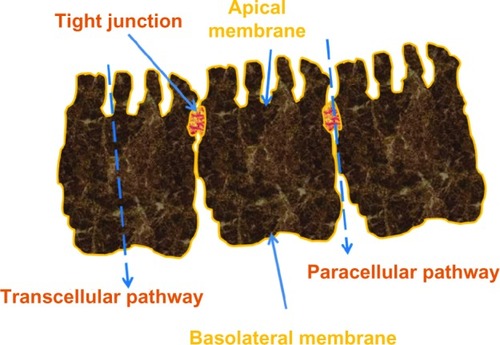
Figure 4 Fasting has been identified as one of the three main reasons for discontinuing treatment.
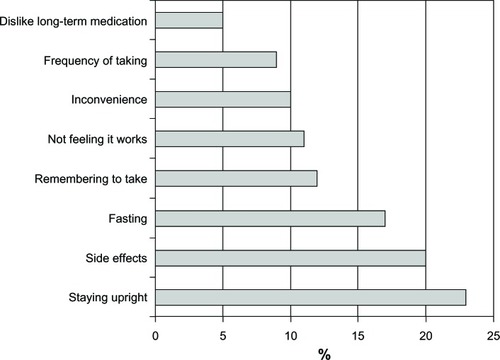
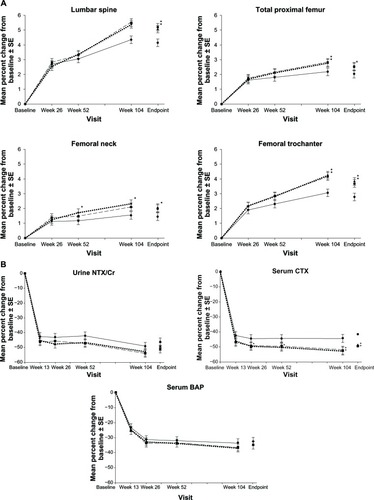
Figure 5 Mean percent change from baseline ± standard error of the mean in (A) bone mineral density and (B) bone turnover markers over 2 years in women receiving risedronate 5 mg immediate-release daily (solid lines with black circles), 35 mg delayed-release immediately following breakfast weekly (dashed lines with black squares), or 35 mg delayed-release at least 30 minutes before breakfast weekly (circle dashed lines with black triangles). Asterisk represents statistically significant difference between immediate-release daily and delayed-release weekly treatment group.
Abbreviations: CTX, C-terminal telopeptide; SE, standard error of the mean; CR, creatinine; BAP, bone alkaline phosphatase.