Figures & data
Figure 1 Different phases of a laparoscopic retrograde aorto-mesenteric bypass to the superior mesenteric artery. (A): Paramedian vertical lines are midclavicular and anterior axial lines. Upper transverse is subcostal, and lower transverse is the line joining the two anterior superior iliac spines. Trocar position 6 for 30° laparoscope, 1 and 9 for aortic clamps and 4, 5, 7 for working instruments. The rest of the trocar positions for other helping instruments. (B): Partially dissected superior mesenteric artery (
 ). Treitz ligament is divided, and duodenum mobilized distally and held under a retractor (
). Treitz ligament is divided, and duodenum mobilized distally and held under a retractor ( ). Inferior mesenteric vein (
). Inferior mesenteric vein ( ). (C): End-to-side anastomosis with superior mesenteric artery. (D): Completed anastomoses on superior mesenteric artery and infrarenal abdominal aorta. Ring enforced expanded polytetrafluoroethylene graft with an end-to-side anastomosed 6 mm graft. Side graft (
). (C): End-to-side anastomosis with superior mesenteric artery. (D): Completed anastomoses on superior mesenteric artery and infrarenal abdominal aorta. Ring enforced expanded polytetrafluoroethylene graft with an end-to-side anastomosed 6 mm graft. Side graft ( ) is being flushed with heparinized NaCl to check the patency of anastomoses before the aortic and superior mesenteric artery clamps are removed. Laparoscopic bulldog artery clamp (
) is being flushed with heparinized NaCl to check the patency of anastomoses before the aortic and superior mesenteric artery clamps are removed. Laparoscopic bulldog artery clamp ( ).
).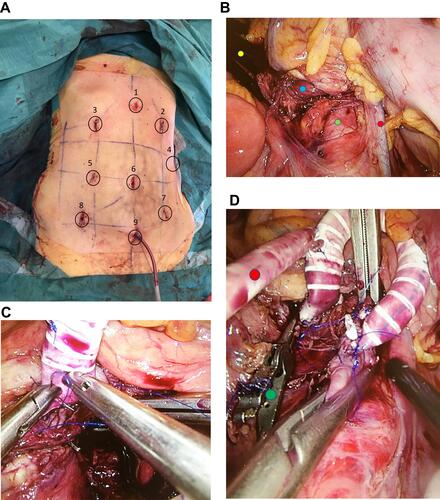
Figure 2 (A). Trocar positions for laparoscopic retrograde aorto-splenic bypass. Trocar positions 5 for 30° laparoscope and 1 for Nathanson’s liver retractor. Position 2, 4, and 3 for working trocars for splenic artery dissection and anastomosis. Positions 7 and 6 for infrarenal aortic dissection and anastomosis. Other positions are used for helping instruments. (B): Distal end of a tunneled ring enforced expanded polytetrafluoroethylene graft anterior to the left renal vein (
 ). (C): Ring enforced expanded polytetrafluoroethylene graft is bein anastomosed end-to-side to a clamped splenic artery. Nathanson’s liver retractor is elevating the left liver lobe. (D): Completed end-to-side anastomosis to the infrarenal aorta.
). (C): Ring enforced expanded polytetrafluoroethylene graft is bein anastomosed end-to-side to a clamped splenic artery. Nathanson’s liver retractor is elevating the left liver lobe. (D): Completed end-to-side anastomosis to the infrarenal aorta.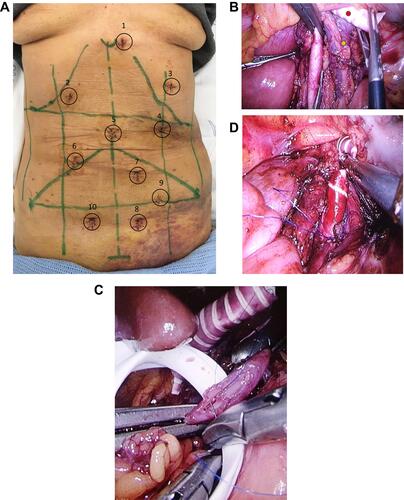
Table 1 Demographic Data, Risk Factors, Comorbidities, and Clinical Findings in the Group of Patients with Chronic Mesenteric Ischemia Treated with Laparoscopic Mesenteric Bypass Procedures
Table 2 Perioperative Data of 9 Chronic Mesenteric Ischemia Patients Treated with Laparoscopic Mesenteric Bypass Procedures
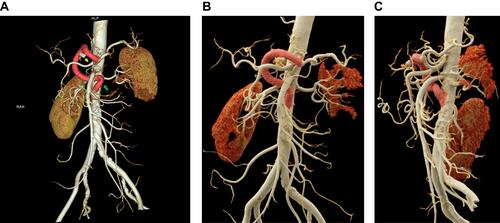
Figure 3 (A). 3D reconstruction of a laparoscopic retrograde aorto-mesenteric bypass to the superior mesenteric artery (yellow arrow). Occluded stent in the superior mesenteric artery (green arrow). (B): 3D reconstruction of a laparoscopic retrograde aorto-mesenteric bypass to the superior mesenteric artery (blue arrow), from the left graft limb of a prior laparoscopic aortobifemoral bypass graft (red arrow). (C): A 6 mm expanded polytetrafluoroethylene graft, end-to-side anastomosed to an 8 mm ring enforced expanded polytetrafluoroethylene graft with graduated length markings and spatulated end.
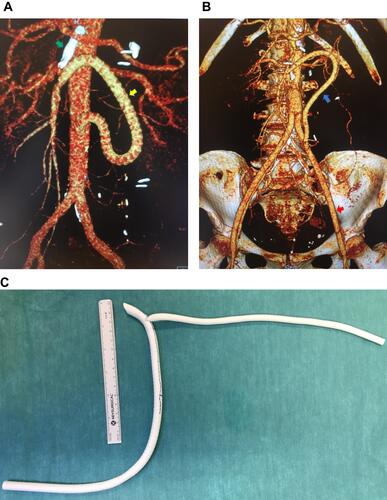
Figure 4 (A). 3D reconstruction of the laparoscopic retrograde aorto-splenic bypass, with graft kinking (green arrow). Hem-o-loc clips on the excised side graft (yellow arrow). (B and C). Anterior and left lateral view of the revised laparoscopic aorto-splenic bypass.