
Figures & data
Figure 1 (A) Hybrid operating room. In the background a table with surgical instruments designed for sternotomy. (B) Cardiac surgical and anesthesia team and an echocardiographer performing TEE monitoring (C) Removed leads. Thick fibrotic tissue with calcific changes around the leads, and a variety of damage to outer silicone tube (mechanical damage during extraction and an old abrasion – dark color of the distal end of the lead). (D) “After the battle”. The tools used for lead extraction: conventional mechanical non-powered sheaths (Byrd polypropylene sheaths, Cook) in three sizes and mechanical rotational threaded sheaths - Evolution (Cook) – two sizes.
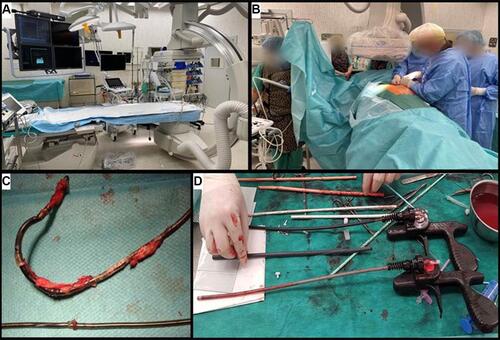
Figure 2 Transvenous extraction of an atrial lead was complicated by right atrial appendage rupture and cardiac tamponade requiring urgent cardiac repair. (A) Fluoroscopy. Atrial lead removal, the tip of the sheath marked with an arrow. (B) 2D TEE images (mid-esophageal view). The winding and pulling on the right atrial appendage (RAA) during extraction of the atrial lead. These potentially harmful effects are not visible on fluoroscopy. The sheath marked with an arrow. (C) 2D TEE images (transgastric view). Separation of pericardial layers – blood – immediately after removal of the lead. (D) Extracted leads on the table. Thick fibrotic encapsulation, partly calcified around the leads. Small abrasion of the external tube with perforation of the atrial lead – less visible. Fluid in the lead in this area. (E) Intraoperative view – RAA rupture/injury.
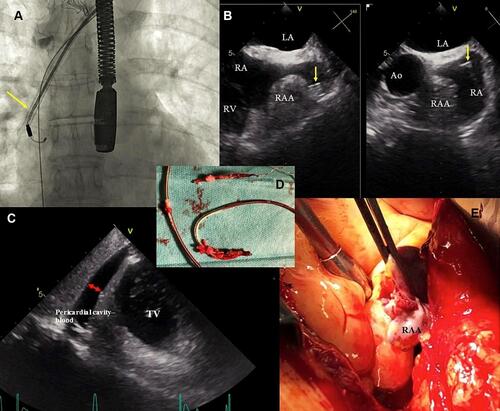
Table 1 Patient Demographic and Clinical Data, Pacing System Data, Indications for TLE
Table 2 Lead Management and Organization of TLE Procedure
Table 3 TLE Procedure Information
Table 4 Effectiveness of Lead Extraction Expressed as Radiographic, Clinical and Procedural Success, Major and Minor Complications in 1000 Procedures
Table 5 Major Complications of TLE in Patients with Lead Implant Duration of Less Than 10 Years
Table 6 List of Publications Describing Effectiveness and Safety of TLE Procedures