
Figures & data
Table 1 Summary of the Salient Epidemiological Characteristics of the ARCADIA, US Fibromuscular Dysplasia (US FMD) Registry and the European/International Fibromuscular Dysplasia Registry and Initiative (FEIRI)
Table 2 Differential Distribution of Clinical Symptomatology of FMD Cohorts
Figure 1 Vascular imaging in a young male patient with a history of right sided amaurosis fugax and right frontal ischemic stroke. Coronal (A) and sagittal (B) views of CT angiogram demonstrate moderate to severe stenosis of the entire right internal carotid artery cervical segment soon after its origin with significant irregularity and beading (white arrows). Anteroposterior (C) and lateral-oblique (D) views on digital subtraction angiogram of right internal carotid artery showed alternate stenosis and dilatation of the extracranial segment (white arrow (C)) and intracranial cavernous-supraclinoid segments (arrowhead (C); white arrow (D)), suggestive of “beading” typical of FMD.
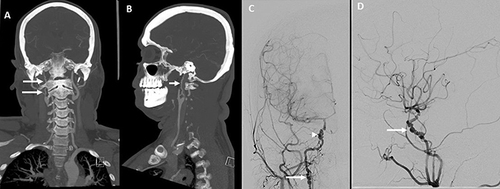
Figure 2 Vascular imaging in a young female patient presenting with acute aphasia and right hemiparesis. Sagittal view (A) on CT angiogram demonstrates mild irregularity with beading in the distal cervical segment of the left internal carotid artery (white arrow) and a dissection in the proximal internal carotid artery soon after the bifurcation seen on axial views (B), white arrow)). Magnified lateral view (C) on digital subtraction angiogram of right internal carotid artery confirms mild “beading” in the distal cervical segment of the carotid.
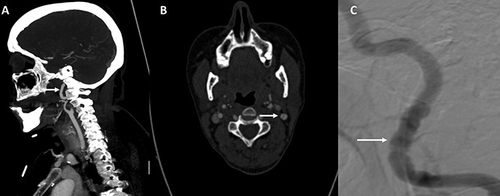
Figure 3 Colour Doppler imaging (A) of the distal internal carotid artery exhibiting the typical pattern of tortuosity and marked turbulence. Colour Doppler imaging (B) showing turbulence and spectral analysis demonstrating high peak velocity (200 cm/s). Colour power angiography (C) demonstrates severe tortuosity of the distal carotid artery with redundancy.
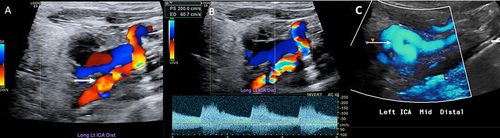
Figure 4 Imaging in a young female with recurrent, left hemispheric strokes despite medical management including antiplatelet therapy. Axial FLAIR MRI brain image (A) shows multiple areas of cortical and subcortical hyperintensity in the left anterior hemisphere. Anteroposterior (B) and lateral (C) views on digital subtraction angiogram of the left carotid bifurcation show a shelf-like ledge along the posterior wall of the proximal internal carotid artery, with minimal intraluminal projection (arrows) without causing significant stenosis. 3-Dimensional rotational angiogram reconstructions (D–F) shows the carotid web circumferentially involving the posterior wall. The patient was treated with carotid artery stenting (G, arrow) and delayed angiogram (H, arrow) shows stasis adjacent to the stent, suggesting the nidus of thrombus formation leading to recurrent stroke in medically managed patients.
