
Figures & data
Figure 1 Patient selection flowchart displays the included and excluded cases as well as the final sample size.
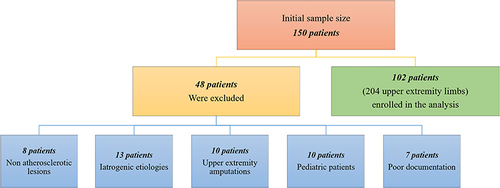
Table 1 Most Common Clinical Presentations in the Study Population (Listed in the Descending Order of Prevalence)
Table 2 Patient Characteristics According to the Segments Affected by Peripheral Arterial Disease
Figure 2 Prevalence and severity of chronic kidney disease (a) and obesity (b) in patients with upper extremity peripheral arterial disease.
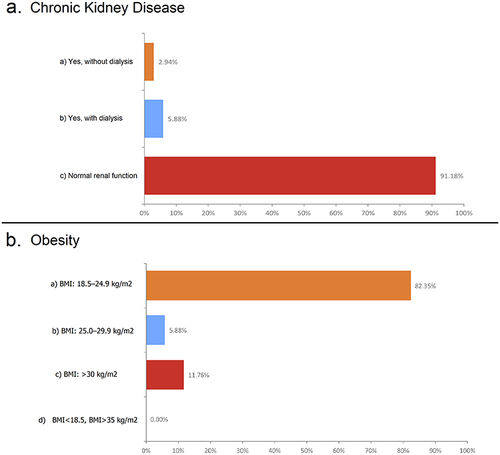
Figure 3 Radiological image from a 47-year-old man with type 2 diabetes mellitus and upper extremity peripheral arterial disease. Three-dimensional, reformatted, volume-rendered computed tomography angiography image shows the high origin of the brachioradial branch (arrow), which represents a higher bifurcation point of the brachial artery. The atherosclerotic and multifocal atherosclerotic segments (arrowheads), leading to attenuated hypoperfusion of the palmar arcs (asterisks), are observed.
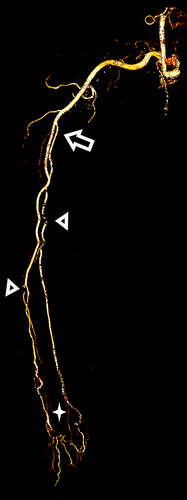
Table 3 Characterization of the Distribution Pattern and Severity of Peripheral Arterial Disease Involvement in Patients with Diabetes Mellitus and in Those with Hypertension
Figure 4 Radiological images from a 45-year-old man with hypertension and upper extremity peripheral arterial disease. The patient reported that the right upper limb felt cold and pained for a week prior to presentation. Upon examination, the radial pulse was absent. (a) A three-dimensional, reformatted, volume-rendered computed tomography angiography (CTA) image acquired from the same patient, with the left arm abducted and externally rotated, shows atherosclerotic changes (arrowheads) with an abrupt cut in the distal part of the brachial artery just before the antecubital fossa (arrow). (b and c) Catheter-directed angiogram confirms the CTA findings of an occluded brachial artery (arrowheads). (d) Further characterization of the distal reconstitution of the radial artery by small collaterals. (e) The thrombus is crossed successfully. (f) The interventionalist used catheter-directed thrombolysis to lyse the thrombus and prevent a distal embolic shower through endovascular manipulation. (g) Final angiographic examination reveals restored flow in the upper right extremities; the patient’s symptoms resolved subsequently. However, a partial filling defect (indicating residual thrombosis) is seen to have persisted in the brachial artery (arrow); this required a more conservative management.
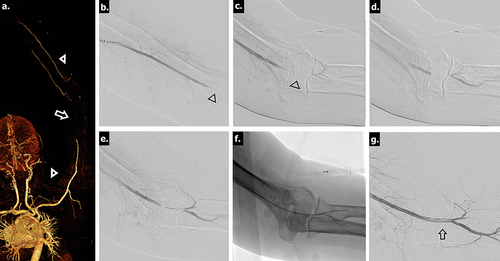
Table 4 Independent Predictors of Total Occlusion Secondary to Peripheral Arterial Disease (PAD) from Among the Patient Characteristics Correlated with Disease Distributiona