
Figures & data
Table 1 Summary of studies from different ethnic and racial groups that disclosed stroke subtype rates
Figure 1 Stroke and extracranial carotid atherosclerosis.
Notes: A man in his 90s came to the hospital with sudden onset of right-sided weakness and difficulty finding words. On exam, he was found aphasic with mild right-sided hemiparesis. (A) A brain magnetic resonance image showed evidence of scattered infarcts over the left hemisphere and a small infarct in the territory of the right anterior cerebral artery. (B) The neck magnetic resonance angiograph showed a flow gap in the left extracranial proximal internal carotid artery (arrow). (C) The brain magnetic resonance angiograph showed the lack of the right proximal segment of the anterior cerebral artery, thus explaining the presence of bi-hemispheric infarcts attributable to left extracranial carotid stenosis through embolization of the anterior communicating artery. (D) A neck artery Doppler confirmed the degree of stenosis (>80%) and the patient underwent carotid endarterectomy and was discharged home after the initial neurological deficits resolved.

Figure 2 Stroke and intracranial atherosclerosis.
Notes: A woman in her 60s came to the hospital for left-sided weakness and headache. On exam, she was found to have mild left pronator drift and visuospatial neglect. (A) The brain magnetic resonance image showed evidence of a right parietal lobe cortical infarct and (B) the brain magnetic resonance angiograph showed evidence of diffuse luminal narrowing of her brain arteries (arrows), with some of these stenoses located proximal to the area of her infarction (small arrow), suggesting artery-to-artery embolism from intracranial large artery stenosis as the most likely stroke mechanism.
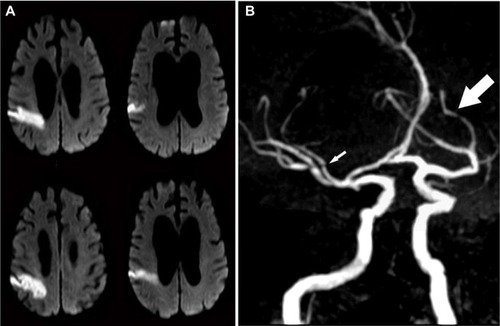
Figure 3 Small artery disease versus branch occlusive disease.
Notes: (A) An example of a small infarct in the left putamen and subcortical white matter (arrow), most likely due to the occlusion of a lenticulostriate artery branching of from the middle cerebral artery. (B) The brain magnetic resonance angiograph in this same patient showed no evidence of large artery stenosis in the proximal middle cerebral artery. (C) A patient with evidence of an infarct (arrow) involving the lenticular nucleus and the head of the caudate nucleus. (D) Contrary to the case presented in A, this patient shows evidence of a high-degree of stenosis in the middle cerebral artery in the brain computed tomography angiograph (large arrow), suggesting branch occlusive disease and “pure” small artery disease as the underling etiology of the infarct.
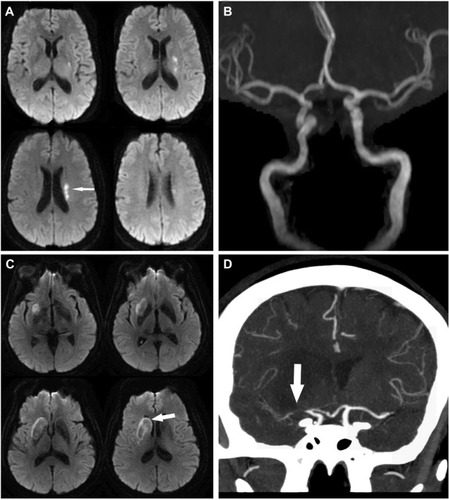
Table 2 Summary of some of the major studies comparing antiplatelets against each other or against placebo in stroke prevention
Table 3 Stroke mechanism and the estimated risk of stroke recurrence in the setting of prevention therapy