Figures & data
Table 1 Revised clinical classification of pulmonary hypertension (Venice 2003)Citation6
Table 2 Modified New York Heart Association classification of functional status in patients with pulmonary hypertension (PHT)
Table 3 Symptoms and signs of pulmonary hypertensionCitation34
Table 4 Patients at risk of developing pulmonary arterial hypertensionCitation37
Figure 1 Proposed algorithm for the medical management of pulmonary arterial hypertension (PAH).Citation41 A positive acute response to vasodilators is defined as a fall in mPAP of at least 10 mmHg to 40 mmHg, with an increased or unchanged cardiac output during acute challenge with inhaled nitric oxide, iv epoprostenol, or iv adenosine. Sustained response to calcium channel blockers is defined as patients being in functional class I or II with near-normal hemodynamics after several months of treatment. Most experts recommend that patients in functional class IV in unstable condition be treated with iv epoprostenol. In patients in functional class III, first-line therapy may include oral endothelin-receptor antagonists, phosphodiesterase inhibitors, long-term iv epoprostenol, or prostanoid analogues.
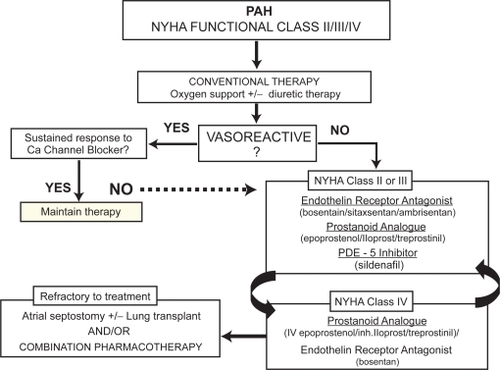
Table 5 Composition and roles of the Royal Perth Hospital PAH multidisciplinary team