Figures & data
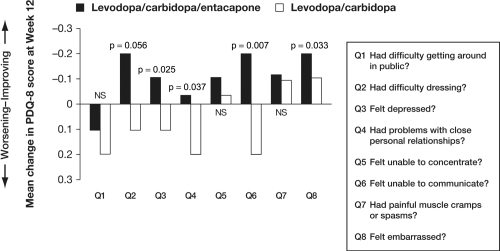
Figure 1 Plasma levodopa profiles with conventional levodopa dosing strategies. Schematic depicting plasma levodopa levels in Parkinson’s disease patients experiencing re-emergence of symptoms due to wearing-off achieved by (A) increasing the daily levodopa/carbidopa dose from 300 mg/day to 450 mg/day; (B)increasing the frequency of levodopa/carbidopa dosing from 3 times/day to 5 times/day.
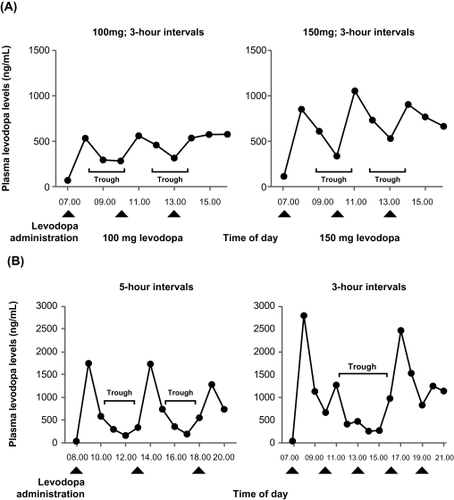
Figure 2 Plasma levodopa profile with levodopa/carbidopa/entacapone versus levodopa/carbidopa. Treatment with levodopa/carbidopa/entacapone 3 times/day significantly improves troughs in plasma levodopa levels compared with equivalent doses of levodopa/carbidopa in patients with Parkinson’s disease; *p < 0.05; †p < 0.01; ‡p < 0.001; SEM, standard error of the mean.
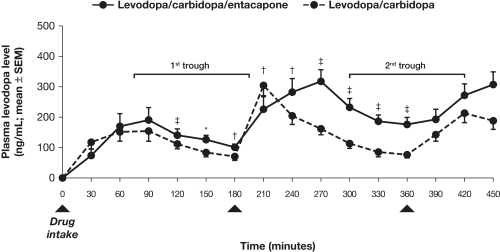
Figure 3 Efficacy of levodopa/dopa decarboxylase inhibitor and entacapone therapy in the short-term. Treatment with levodopa/DDCI and entacapone is associated with significant improvements in functional control as determined by UPDRS total, ADL and motor scores compared with levodopa/DDCI and placebo over 6 months. *p < 0.01; †p < 0.05.
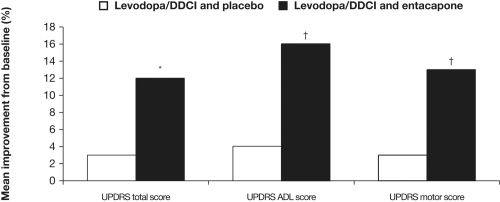
Table 1 Most frequent adverse events associated with levodopa/dopa decarboxylase inhibitor and entacapone therapy
Figure 4 Efficacy of levodopa/dopa decarboxylase inhibitor and entacapone therapy in the long-term. Functionality is maintained over three years with levodopa/DDCI and entacapone.
‡p =not significant.
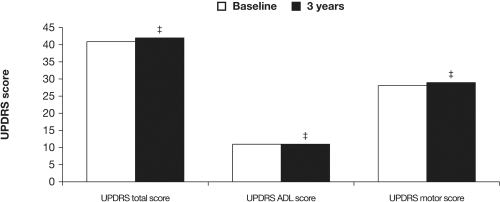
Figure 5 Effect of levodopa/carbidopa/entacapone on quality of life in patients with stable Parkinson’s disease. Treatment with levodopa/carbidopa/entacapone is associated with significant benefits in terms of quality of life compared with levodopa/carbidopa, as determined by the Parkinson’s disease questionnaire-8.