Figures & data
Figure 1 (A–C) Typical contractural aracnodactylia in Beals syndrome (A, B) and joint hypermobility (C).
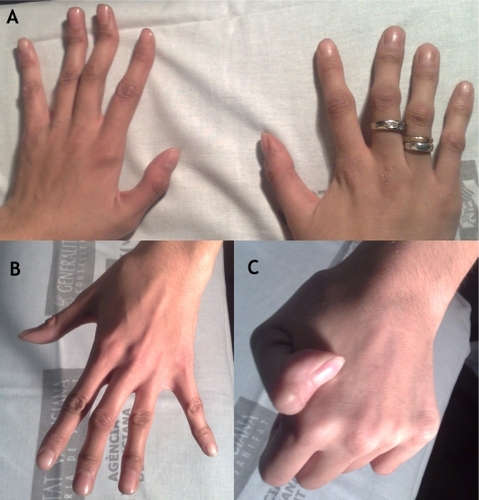
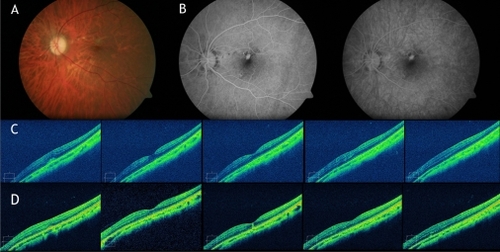
Figure 2 Fundus examination. A) Retinography showing disciform-like scar RE and juxtafoveal fibrovascular proliferation LE. B) Angiogram showing predominantly classic choroidal neovascular membrane (CNV). C) Spectral-domain optical coherence tomography (SD-OCT) images showing the subretinal choroidal neovascular membrane inducing loss of foveal anatomy. D) SD-OCT images showing complete resolution of the retinal edema and normalization of the foveal anatomy after three monthly intravitreal ranibizumab injections.