Figures & data
Table 1 Preoperative data of lower eyelid retraction patients
Figure 1 Figure 1A A 3-mm left lower eyelid retraction caused by previous surgery for a squint (inferior rectus muscle recession) is shown.
Figure 1B The anterior surface of the lower eyelid retractors is shown. Part of the Lockwood ligament can be seen.
Figure 1C The posterior surface of the lower eyelid retractors is shown. The double layers of the retractors can be clearly discerned. The posterior layer of the lower eyelid retractors is always shorter than the anterior layer.
Figure 1D The lateral and medial horns of the lower eyelid retractors are incised at the width of 17 mm.
Figure 1E The harvested auricular cartilage is interposed between the lower edge of the tarsus and the distal edge of the anterior layer of the lower eyelid retractors while the posterior layer remains unfixed to any structure. The volume of the harvested cartilage for the retraction patients is twice the retraction from the lower corneal limbus with 1 mm of extra volume in the proximal and distal margins, respectively, for sutures. The height of the harvested cartilage for the entropion patients is 4 mm (horizontal length in both groups is always constant at 17 mm).
Figure 1F The cartilage is fixed with 5 sutures on each of the distal and proximal sides. The suture on the right upper edge is masked by the recessed anterior layer of the lower eyelid retractors in this image.
Figure 1G Sufficient elevation of the lower eyelid is shown. The skin is sutured with interrupted 6–0 nylon sutures.
Figure 1H The rehabilitated left lower eyelid moves down sufficiently during a downward gaze.
Figure 1I The contour of the left lower eyelid is within the permissible range.
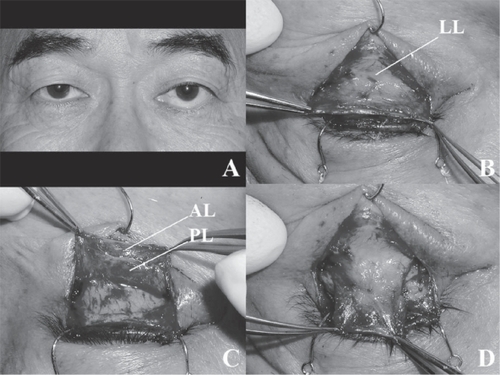
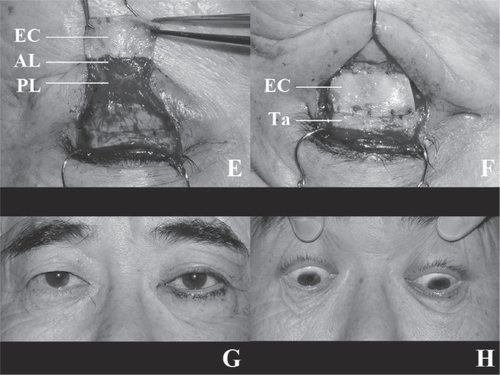
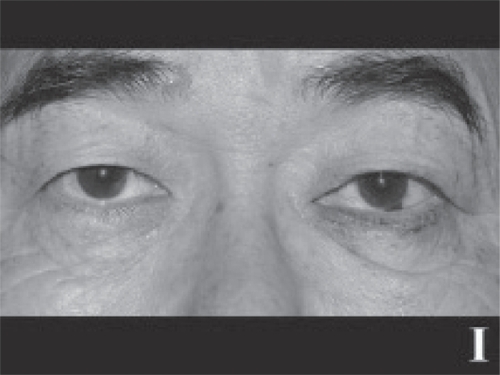
Figure 2 Figure 2A The patient shows 5-mm right and 4-mm left retractions from the lower corneal limbi with proptosis of 26 mm OU. Just the right lower eyelid took two Hotz procedures for the lower eyelid entropion.
Figure 2B After lower eyelid lengthening surgery, the right lower eyelid retraction and cicatricial entropion are sufficiently improved.

Table 2 Postoperative data of lower eyelid retraction patients