Figures & data
Figure 1 Computed tomography of the coronal view demonstrating the blockage of the ostiomeatal complex. A medial mass lesion at the lacrimal sac is noted. A bony osteium in the lacrimal bone is apparent from the first initial external dacryocystorhinostomy providing patency into the nasolacrimal duct.
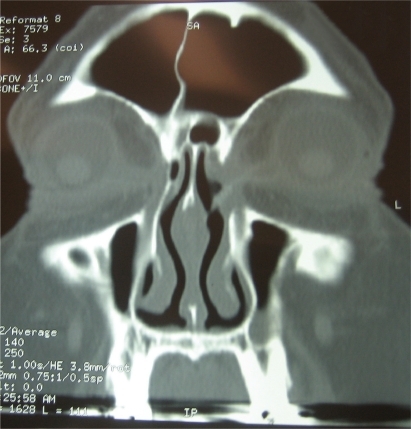
Figure 2 Nasoendoscopic view of bony nasal lacrimal canal. The canal is formed by the maxilla, the lacrimal bone and the inferior nasal concha.
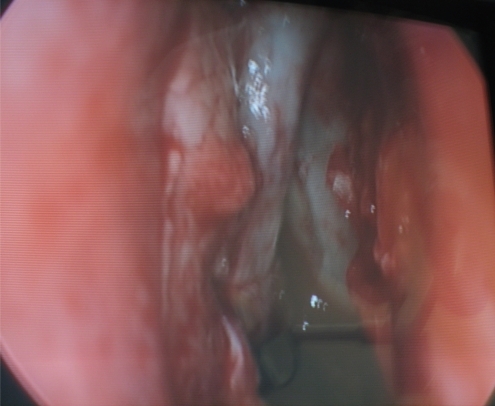
Figure 3 Gross specimen postsurgical resection of lacrimal apparatus. Upper and lower lid canaliculi are visible with probes in situ. The lacrimal sac and duct was resected intact and the gross specimen sent for histopathology.

Figure 4 Nasal lacrimal apparatus postfixation with formula for histopathology. Correct anatomical orientation. The lacrimal sac measured about 20-mm long and connected to the inferior meatus of the nose by the nasolacrimal duct. The direction of the duct is downward, backward and lateral is lodged in the bony nasolacrimal canal.

Figure 5 Hematoxylin and eosin stain with low power magnification of the nasolacrimal sac. This was lined by a malignant papillary epithelial tumor. The tumor was mostly noninvasive with isolated foci of stromal invasion.
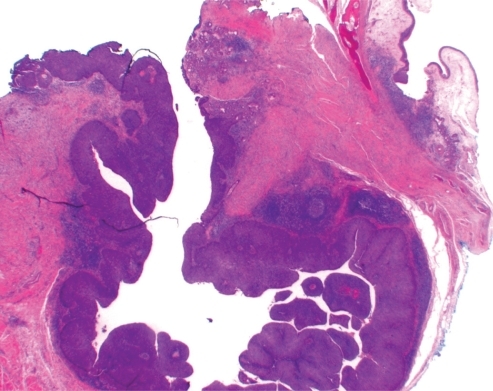
Figure 6 Higher power magnification (hematoxylin and eosin stain x80). Distinct features of transitional cell carcinoma were noted on microscopy with focal squamous differentiation (nonkeratinising cell carcinoma) High grade in situ carcinoma extended superiorly along both lacrimal canaliculi and inferiorly along the nasolacrimal duct. All margins were clear with appearance of complete excision.
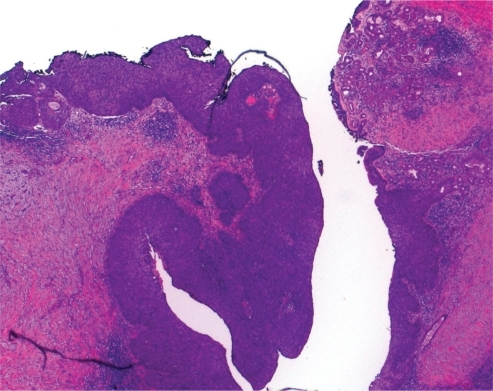
Figure 7 Ten days postoperative follow-up: satisfactory cosmetic result.

Figure 8 Ten days postoperative follow-up: satisfactory cosmetic result.
