Figures & data
Figure 1 Short-axis view of LV from the two diabetic women with MRI-visible subendocardial infarction (arrow). In the patient with multi-vessel disease (left panel) the location of subendocardial MI is inferior while the patient with normal coronary angiogram (right panel) had smaller subendocardial MI located in the anterior LV wall.
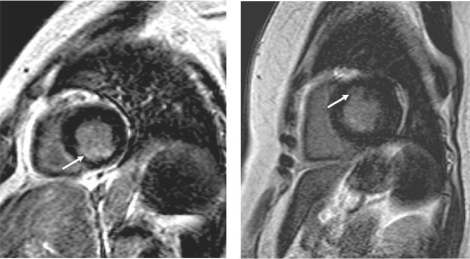
Table 1 Basic characteristics
Table 2 LV systolic function and morphology
Figure 2 Normal coronary angiogram from the patient with small anterior subendocardial infarction. This patient had recently diagnosed diabetes mellitus. Coronary angiography did not revealed any signs of obstructive atherosclerotic plaque in the large epicardial arteries. (Left panel) left anterior oblique view of the right coronary artery. (Right panel) Right anterior oblique view of left anterior descending artery (LAD) and left circumflex artery (LCx).
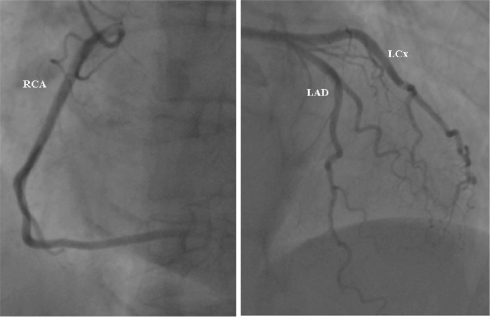
Figure 3 Coronary angiogram from the patient with inferior subendocardial infarction. There is evidence of multivessel disease. The images depicts occluded (arrow) right coronary artery (RCA) (left panel) and multiple significant stenosis (>50 % of reference lumen diameter) (arrows) in left anterior descending artery (LAD) and left circumflex artery (LCx) (right panel).
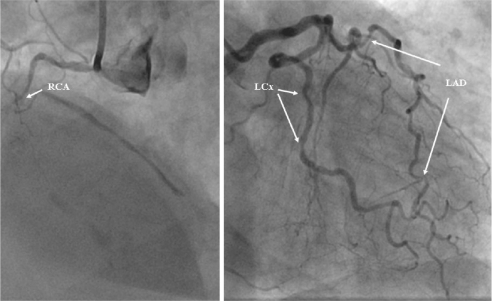
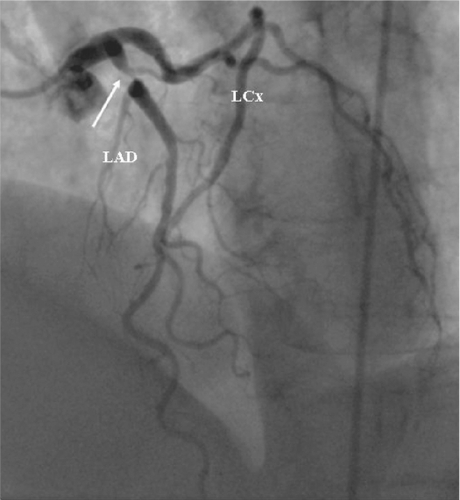
Figure 4 Coronary angiogram from the patient diabetes mellitus with developed unstable angina one week after that magnetic resonance imaging investigation suggested presence of significant coronary disease. Notice tight narrowing (arrow) in the proximal segment of left anterior descending artery (LAD).