Figures & data
Figure 1 ACC/AHA Guidelines for Cardiovascular Risk Reduction in Patients with peripheral arterial disease. Reproduced from CitationHirsch AT, Haskal ZJ, Hertzer, HR, et al. 2006. ACC/AHA Guidelines for the Management of Patients with Peripheral Artery Disease: Executive Summary. J Am Coll Cardiol, 47:1239–312. Copyright © 2006 with permission from Elsevier.
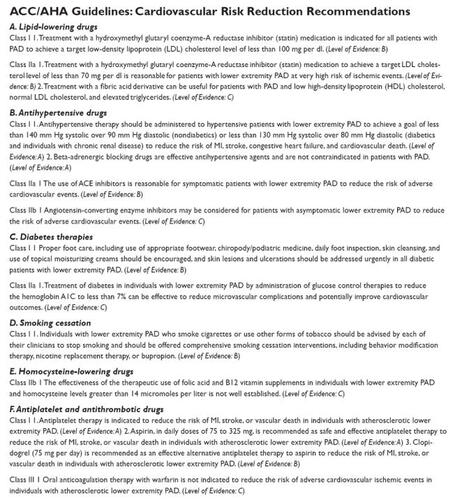
Figure 2 Platelet interactions with diseased endothelium. Endothelial dysfunction, a consequence of a variety of disease states, has important implications for platelet aggregation and vascular tone. When platelets aggregate, they release thromboxane A2 (TxA2), 5-hydroxytryptamine (5-HT, or serotonin), and ADP.
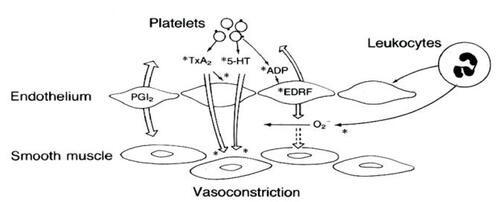
Figure 3 Clopidogrel molecule.
Figure 4 Fatal or non-fatal vascular events in the CAPRIE Study. Reproduced from CAPRIE Steering Committee. 1996. A randomized, blinded, trial of clopidogrel versus aspirin in patients at risk of ischemic events (CAPRIE). Lancet, 348:1329–39. Copyright © 1996 with permission from Elsevier.
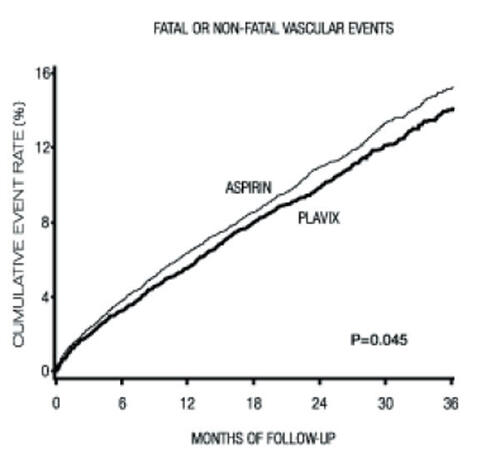
Table 1 Classificaton of peripheral arterial disease
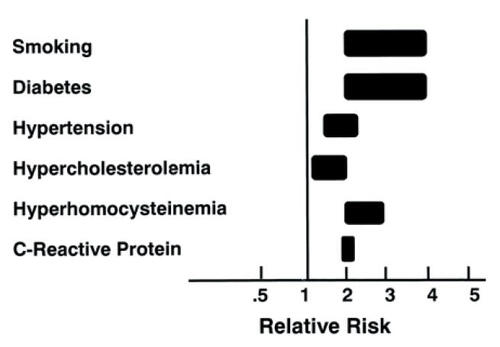
Figure 5 Risk of developing lower extremity peripheral arterial disease. The range for each risk factor is estimated from epidemiologic studies (see text). The relative risks take into consideration current smokers vs. former smokers and nonsmokers; the presence vs the absence of diabetes and hypertension; and the highest vs. the lowest quartile of homocysteine and C-reactive protein. The estimate for hypercholesterolemia is based on a 10% risk for each 10 mg/dL rise in total cholesterol. Adapted from CitationDormandy JA, Rutherford RB. 2000. Management of peripheral arterial disease (PAD). TASC Working Group. TransAtlantic InterSociety Consensus (TASC). J Vasc Surg, 31:S1-S296. Copyright © 2000 with permission from Elsevier.