Figures & data
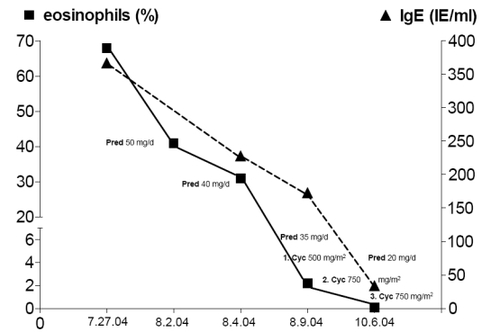
Figure 1 Angiogram of the left coronary artery. The left anterior descending coronary artery (LAD) is distally occluded (arrow in A); after intracoronary application of nitroglycerine the LAD is open (arrows in B), but demonstrating a long, severely diseased coronary segment that is significantly stenosed. Because of the long coronary segment involved, the small diameter and the suspicion of inflammatory origin of the stenosis, percutaneous coronary intervention was not attempted.
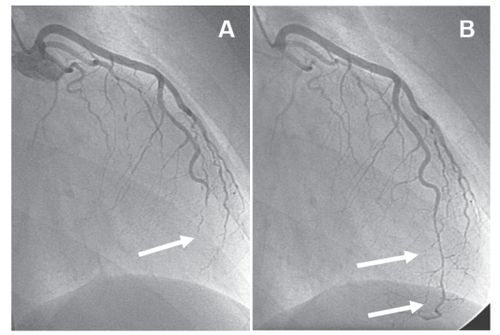
Figure 2A Magnetic resonance imaging of the left ventricle. Phase sensitive T1-weighted contrast based late enhancement sequence (PSIR). A subendocardial bandlinke hyperintensity in the interventricular septum was found in the four chamber view and short axis orientation (arrow). A small pericardial effusion was present.
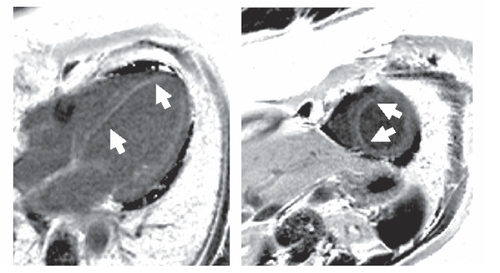
Figure 2B Follow-up after four months. Subendocardial late enhancement persisted, though smaller in extension as seen in this PSIR late enhancement image of the four chamber view and short axis orientation. No pericardial effusion.
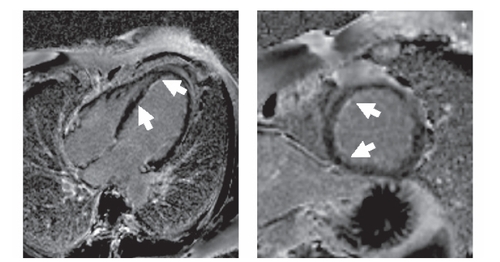
Figure 2C After 12 months, further reduction of the basal septal late enhancement area was present, however there is persisting late enhancement in the apical septum with wall thinning.
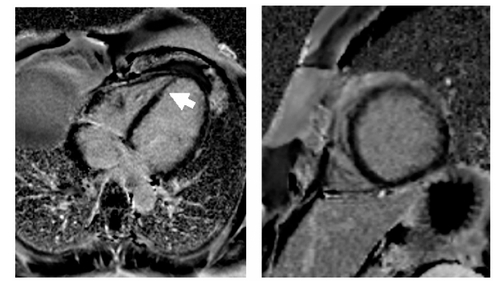
Figure 3 Eosinophils and creatine kinase (CK) levels during three months follow-up. In August 2004 prednisolone 50 mg daily was administered. The eosinophils and CK levels decreased continuously under prednisolone treatment.