Figures & data
Table 1 Relaxivity (r1) in human plasma at 37 °C (mM-1s-1)
Figure 1 Gadofosveset-enhanced MRA data of a 30-year old healthy proband: after contrast agent injection and by using new multi-channel MR scanners, a MRA in dynamic or first-pass phase with purely arterial contrast can be realized for both the carotid arteries and the lower thigh arteries (A, spatial resolution: 1.0 mm3 voxel size, subtracted maximum-intensity projections (MIP), acquisition time: 29 seconds). In the following acquisition performed during the equilibrium phase, very high spatial resolutions of below 0.1 mm3 voxel size can be achieved, which, at a satisfactory signal-to-noise ratio, permit sufficient differentiation between arterial and venous vascular structures despite the small vascular diameter and the close proximity of the structures (B, C (enlarged view), 0.074 mm3 voxel size, acquisition time: 6:15 minutes, arrows: veins; arrow heads: arteries). Image: courtesy Konstantin CitationNikolaou, reproduced from Mathias Goyen (ed.). 2006. Vasovist – the first intravascular contrast agent for MR angiography. ABW-Wissenschaftsverlag Berlin.
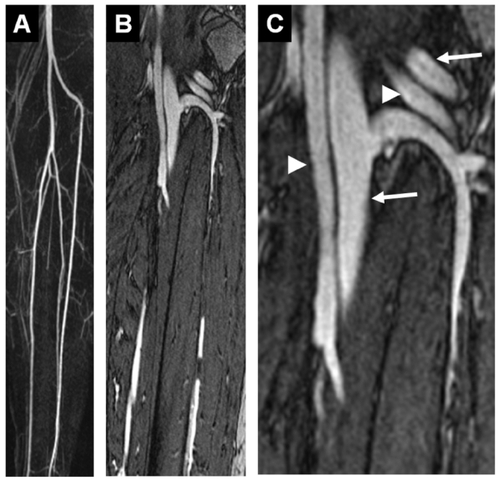
Figure 2 Example of a healthy proband whole-body MRA: compilation of a gadofosveset-enhanced whole-body MRA with acquisition of the carotid arteries (A) and the lower thigh arteries (B) in the dynamic and first-pass phase (for acquisition parameter refer to ), as well as acquisition of the thoracic area (C, voxel size 1.0 mm3, acquisition time: 37 seconds), abdomen (D, voxel size 1.0 mm3, acquisition time: 35 seconds). The signal-to-noise ratio that can be achieved in the equilibrium phase is even sufficient for satisfactory imaging of the coronary arteries (E, voxel size: 0.7 mm3, navigator technology, acquisition time: 3:30 min). Ao: aorta; arrow: right coronary artery. Image courtesy Konstantin CitationNikolaou, reproduced from Mathias Goyen (ed.). 2006. Vasovist – the first intravascular contrast agent for MR angiography, ABW-Wissenschaftsverlag Berlin.
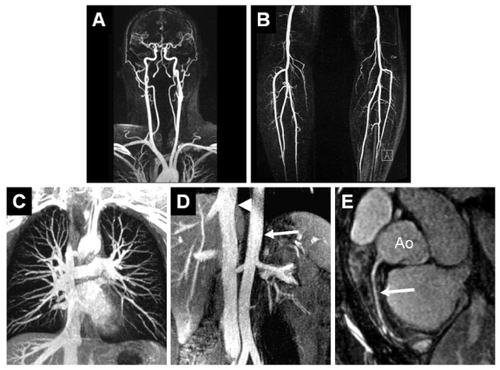
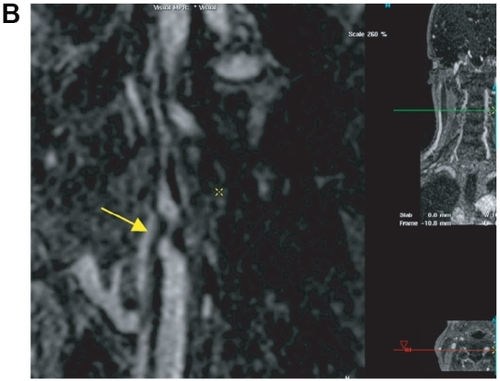
Figure 3 Sixty-four-year-old male presented with known peripheral vascular disease. The MRA suggests an occlusion of the fibular artery at the level of the distal calf on the first-pass image: the vessel cannot be identified even on the curved MPR (A) due to venous overlay (A). However, curved MPR of the higher spatial resolution steady-state images (B allows for clear identification of the distal fibular artery next to the fibular vein and allows for depiction of the distal collateral filling of the posterior tibial artery. Image courtesy Winfried Willinek, Department of Radiology, University of Bonn/Germany).

Figure 4 Patient with symptomatic abdominal aortic aneurysm referred for peripheral MRA. The high grade stenosis of the left internal carotid artery was confirmed by 64 multi-slice CTA and the patient was discharged after successful thrombendarterectomy and aneurysm repair. After first-pass MRA of the abdomen and lower extremities (A), an ultra-sonographically suspected stenosis of the left internal carotid artery is confirmed by the 0.66 mm isotropic resolution steady-state gadofosveset-enhanced MRA (B, arrow). This approach facilitates the pre-operative work-up of patients with systemic vascular disease without the need of a second contrast injection or a separate MR-examination. Image courtesy Winfried Willinek, Department of Radiology, University of Bonn/Germany.