Figures & data
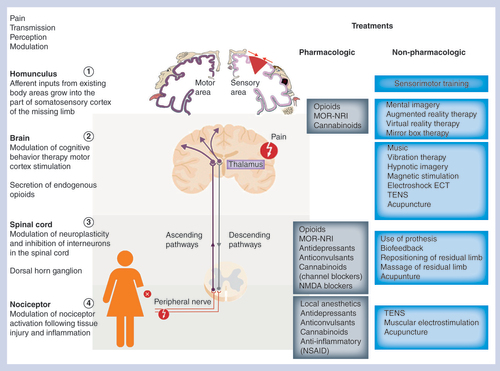
Diagram showing the sites of action of different categories of pharmacologic and nonpharmacologic treatments, as well as their potential in the modulation of pain between the peripheral nervous system and CNS (brain and spinal cord). From the site of injury, such as an amputation, nociceptors send signals to the spinal cord (transduction) and then to the brain (transmission) through the ascending pathways where the pain is treated (perception). Pain signal is then modulated through the descending pathways. On the left hand side of the figures are mentioned the different parts of the human body that are implicated in the pain pathway from the site of injury to the homunculus in the brain via the spinal cord. On the right hand side of the diagram, the different options among pharmacological and nonpharmacological treatments are listed as well as their known sites of action along the signaling pain pathway.
NSAID: Non-steroidal anti-inflammatory drug; TENS: Transcutaneous electrical nerve stimulation.
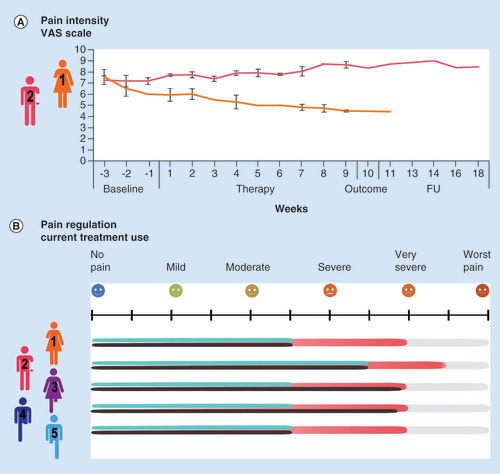
Evaluation of pain intensity (visual analog scale) 24 h before the beginning of therapy sessions by electrical stimulation was done for the two patients who participated in the study under the EPIONE protocol. The 3-month study period was divided into a 3-week baseline phase (control measures), a 9-week therapy phase with electrical stimulation sessions three-times per week, a 1-week period for evaluation of the outcome and, finally, a follow-up period to assess the long-term effect of the therapy. At each session during the successive phases of the protocol, patients 1 and 2 were asked to score their highest experienced pain level before the session using the software platform (A). The intensity of pain (from severe pain to no pain, red bar) was estimated for each patient according to their respective testimonies, as well as the impact of pharmacological (black bars) or nonpharmacological treatments (blue bars) on their pain relief (B).
VAS: Visual analog scale.
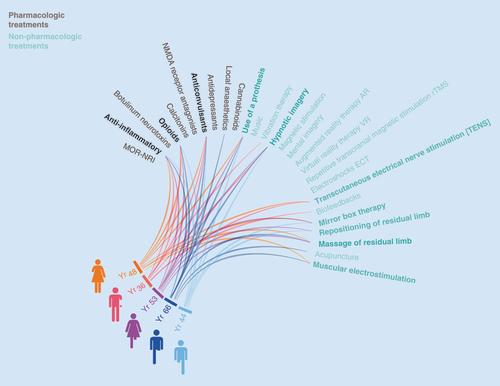
The diagram illustrates the vast therapy options that could be proposed to patients suffering from phantom limb pain. Among those different therapeutic strategies, the five patients have been treated according to conventional pharmacologic agents, such as anti-inflammatory, opioids and anticonvulsants drugs (black letters on the left). Currently available nonpharmacologic treatments (blue letters) to combine with the pharmacologic options are listed on the right and therapeutic options commonly tested by the five patients are highlighted.
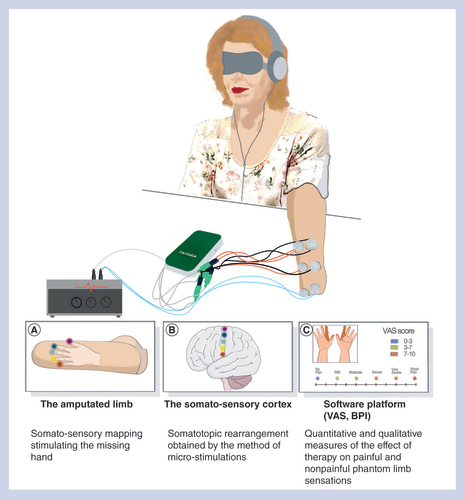
One part of the European EPIONE project is based on a noninvasive approach of transcutaneous electrical stimulations in order to create nonpainful sensations to the amputated patient suffering from phantom limb pain (A) and therefore alleviate the pain intensity by restoring neuroplastic changes in the cortex (B). A software platform was developed in order to quantitatively and qualitatively follow the effect of the therapy on the painful and nonpainful phantom limb sensations, as well as the psychological state of the patients through multiple questionnaires (C).
VAS: Visual analog scale.
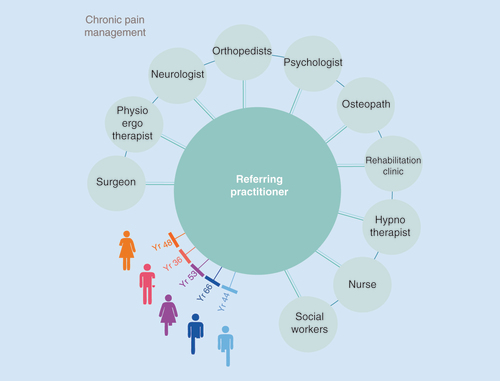
To assure that the patient suffering from chronic pain has an optimal and personalized therapeutic plan, a specialist’s network is needed with the patient in the center. At the center of the figure and directly linked to the patient is the referring specialist who is responsible to maintain the main therapeutic plan, as well as the discussion network in the multidisciplinary specialists team potentially involved in the pain management whatever the moment or the evolution of the pain.