Figures & data
Figure 1. Dose distributions in the sagittal and transversal plane related to treatment with (from left) 3D CRT, RapidAarc and IMPT.
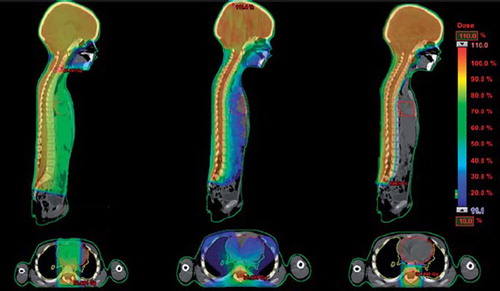
Table I. Organ-specific dose objectives relating to children treated with radiation therapy.


Table II. Radiation-related secondary cancer incidence from the lSS [Citation34] and as adopted in this study. the incidence is given as average excess absolute risk due to external low-lEt radiation as per 10 000 person years and Sieverts equivalent dose.
Table III. Dose-response functions and corresponding model parameters utilized in the estimation of treatment-induced non-cancer adverse effects.
Figure 2. Mean values for all 10 patients of cumulative solid secondary cancer risk as a function of attained age for the three different treatment modalities studied. Results are given for the two different prescription CSI dose levels that are relevant for this patient group. The results are shown up to an attained age of 100 years, after this the cumulative risk levels out since the probability of surviving to older ages is very low. For IMPT the results are given as including SN dose with values of the WRneutron as proposed in ICRP publication 92, denoted IMPT_SN and values five times higher, denoted IMPT_SNx5.
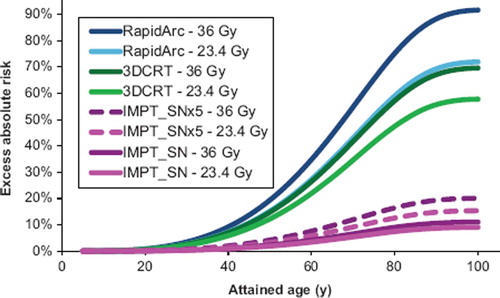
Figure 3. Mean values of EAR are given for a plateau, bell shape and a linear model, normalized to the EAR of the plateau model. The estimates are given for prescribed CSI doses of a) 23.4 Gy and b) 36 Gy. The relative difference between models depends on the initial slope of the dose-response curves and at what doses the risk plateaus out/turns over. The linear model deviates somewhat from the other two, likely since it did not provide a good fit to the original input data.
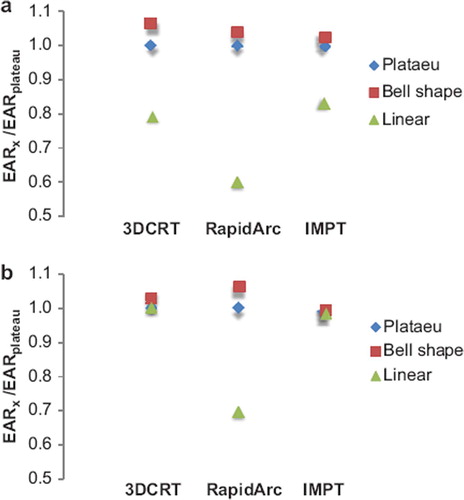
Figure 4. Mean values for all 10 patients comparing long-term risks of inducing pneumonitis, heart failure, xerostomia, blindness, hypothyroidism and ototoxicity between the different treatment modalities.
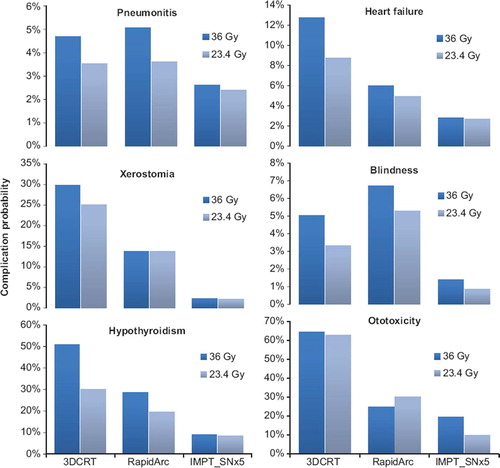
Figure 5. Mean values of all 10 patients comparing the risk of heart failure for different spinal field widths in 3D CRT treatment.
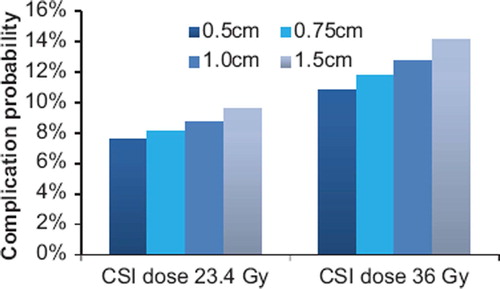
Table IV. Mean values for all ten patients of target coverage parameters comparing the 3D CRT, RapidArc and IMPT plans for the 23.4 Gy craniospinal prescription dose.