Figures & data
Table I. Outcomes and toxicity rates for various head and neck cancers treated with radiation therapy.*
Figure 1. This shows a comparison of an intensity-modulated radiotherapy (IMRT) plan and a proton therapy (PT) plan for a 46-year-old female with a spindle cell carcinoma involving the right maxillary sinus (pT4N0) with involvement of the infraorbital nerve, the orbit, the pterygomaxillary space, and the infratemporal fossa, status post endoscopic maxillectomy, rhinotomy, and orbital decompression. For both plans, the prescribed dose to the primary target was 74.4 Gy/CGE in 1.2 Gy/CGE twice-daily fractions. The low neck was also prescribed 50 Gy in 2 Gy fractions with 6 MV photons with concurrent weekly cisplatin during radiation therapy.
shows color-wash depictions of the dose distributions achieved with the PT plan (left) and the IMRT plan (right). As apparent from the axial, coronal, and sagittal images, there is greater integral dose with the IMRT plan. shows the dose-volume histogram (DVH) comparison between the two plans; as apparent from the curves on the far right, the target coverage was the same for the two plans, but the PT plan delivered a significantly lower dose to the optic structures, including the chiasm, the lacrimal glands, the retinae, and the optic nerves as well as the brainstem and parotids. The differences in dose to these structure are further detailed in .
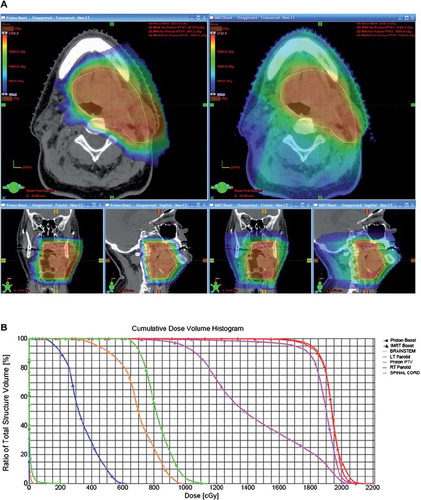
Table II. Comparison of normal-tissue exposure between IMRT and PT plans* for sinonasal carcinoma.
Table III. Guidelines and specific considerations in treatment planning of proton therapy.