Figures & data
Figure 1. Histological findings of LCH in the right supraclavicular lymph node of Case 6. (1) The node is extensively infiltrated by coalescent, focally necrotized infiltrates with prevailing sinusoidal distribution (a – LCH infiltrates, b – lymph node tissue, c – necrotic foci, d – lymph node capsule). (2) The lesional cells have bland lobular nuclei frequently with indentations and abundant cytoplasm (a – Langerhans cells with reactive eosinophils, b – eosinophilic abscess with necrosis, c – giant multinucleated cells). The immunohistochemical staining causes brown membrane (3) and brown nuclear and cytoplasmatic (4) colorings. White scale line = 50 μm.
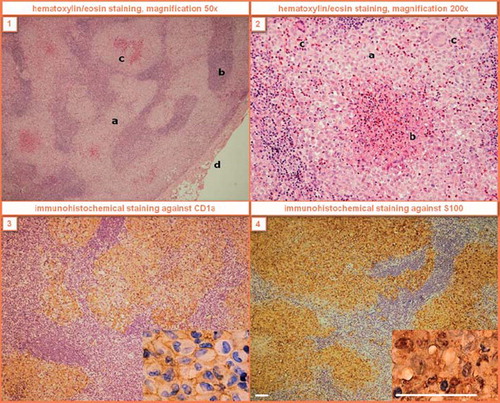
Figure 2. T1 weighted MRI scans of the brain in transverse (left) and sagittal (right) planes after application of contrast agent in Case 2. Due to incipient eyesight deterioration and increased tracer uptake in the occipital region on bone scintigraphy, the patient was sent to MRI which revealed an osteolytic lesion infiltrating the meningeal membranes near the occipital lobe. The function of the centre of vision which is located in the occipital lobe was deteriorated in this patient by intracranial propagation of LCH. After cladribine treatment the infiltration receded, which was followed by a complete vision recovery.
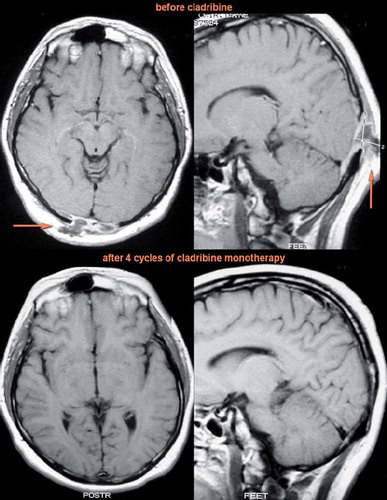
Table I. Main demographic and clinical characteristics of seven patients treated with cladribine.
Table II. An overview of cladribine-based treatment and therapy responses in seven adult patients with LCH.
Figure 3. T1 weighted MRI scans of the brain in coronary (left) and sagittal (right) planes after application of contrast agent in Case 3. The ball-shaped enlargement (infiltration of the hypophysis infundibulum by LCH) fully retreated after cladribine monotherapy.
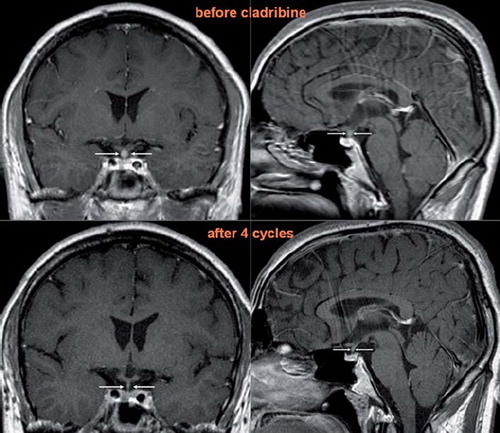
Table III. Hematological treatment-related toxicities during the cladribine-based treatment.