Figures & data
Figure 1. Tubular silver catheters devised by Ambroise Paré (1510–1590), with long gentle curves (they are known as coudé catheters) to permit easier insertion [Citation8].
![Figure 1. Tubular silver catheters devised by Ambroise Paré (1510–1590), with long gentle curves (they are known as coudé catheters) to permit easier insertion [Citation8].](/cms/asset/cb80016f-8a8a-4666-a3ad-29c960496f29/ijmt_a_1085600_f0001_b.jpg)
Figure 2. Urinary catheterization in the middle ages [Citation17].
![Figure 2. Urinary catheterization in the middle ages [Citation17].](/cms/asset/fab0c956-15cf-4d69-a821-fe955089d3b1/ijmt_a_1085600_f0002_b.jpg)
Table 1. Some important events in the history of the development of the urinary catheter.
Figure 3. The urinary tract.
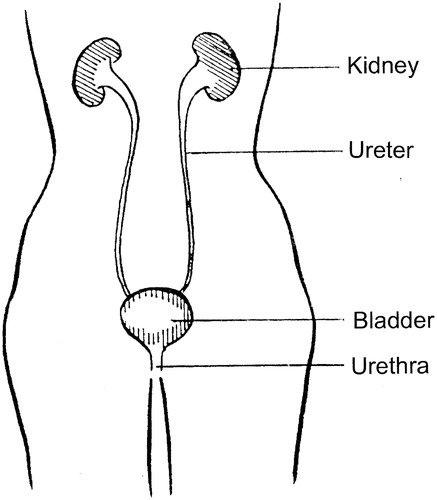
Figure 4. A typical Foley catheter. This catheter is size 16 Fr. Its overall length is ∼400 mm and the volume of the fully-inflated balloon is ∼10 ml. The catheter has two channels. When the catheter has been inserted, the retaining balloon is inflated with sterile water from a syringe via the inflation connector and one of the channels. The inflation connector incorporates a valve to prevent the sterile water from escaping when the syringe is detached. The other channel allows the free flow of urine from the drainage eye to the drainage funnel. To remove the catheter, the retaining balloon is first deflated by withdrawing the water from it with a syringe, which opens the valve in the inflation connector when it is attached.
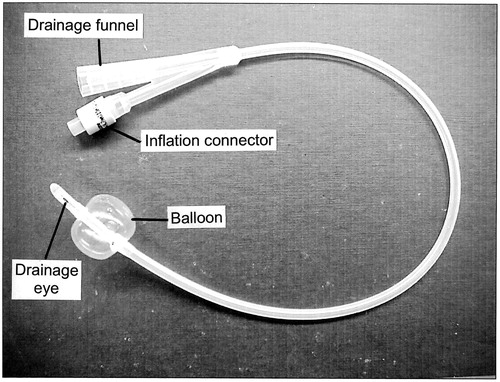
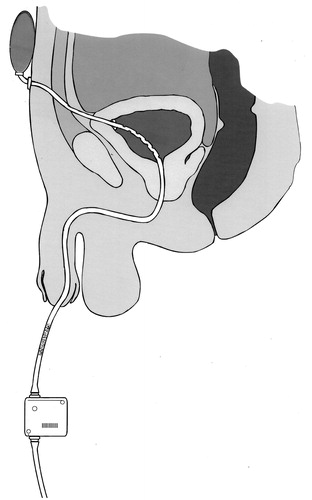
Figure 5. The Foley catheter, introduced (a) Urethrally and (b) Suprapubically. In both cases, the bladder is shown to be draining continuously into a urine collection bag attached to the leg: this bag can be emptied when necessary by opening a valve. Alternatively, the bladder can be drained intermittently if a catheter valve is inserted into the drainage funnel of the catheter.
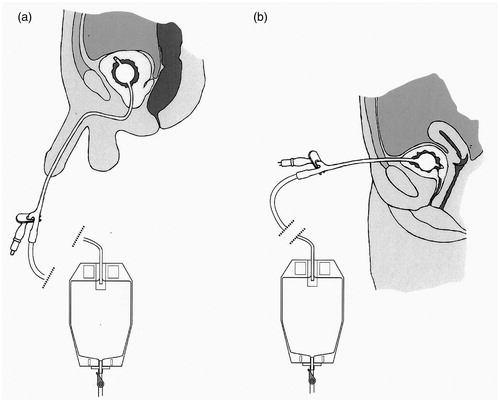
Figure 6. A section through a Foley catheter that has become blocked during use by the formation of struvite. The smaller patent lumen is the channel for the inflation and deflation of the retaining balloon. The length of the scale bar is 1 mm.

Figure 7. A catheter incorporating some of the concepts in the research agenda. The catheter is retained by wings which spring open after insertion through the suprapubic tract to the bladder: this traps less urine than the balloon of a Foley catheter and the catheter can be withdrawn transurethrally after cutting through it at the external suprapubic port. Multiple drainage eyes in the section of the catheter within the bladder minimize the risk of the formation of pseudopolyps, and this risk is further reduced by a collapsible section (shown stippled) of the catheter situated close to the external meatus of the urethra. The elastic reservoir at the suprapubic end of the catheter and strapped to the abdominal wall expands to accommodate urine from the bladder during spasmodic bladder contraction and returns it to the bladder when it relaxes after the spasm, thus minimizing the possibility of kidney damage. Periodic drainage of the bladder into a leg bag is actuated by a pinch valve beyond the collapsible section of the catheter, under manual or timed automatic control.