Figures & data
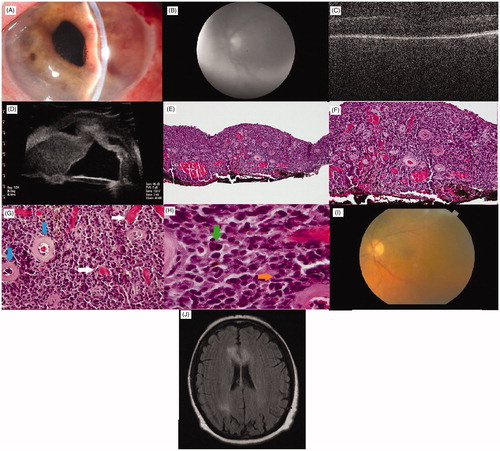
FIGURE 1. (A) Slit lamp photograph of anterior segment of left eye prior to surgery. Note raised contour of iris and keratic precipitates. Note also temporal iris neovascularization. (B) Red free photograph of fundus of left eye prior to surgery. Poor view secondary to keratic precipitates and vitreous debris. (C) OCT of the macula of the left eye prior to surgery. (D) Ultrasound showing thickened iris stroma actually touching cornea. E–H. Representative light photomicrographs of a diffuse lymphoproliferative infiltration of the iris stroma, involving the entire specimen. The infiltrate consists of large lymphocytes demonstrating malignant features including pleomorphism, high nuclear:cytoplasmic ratios, clumped chromatin and rare nucleoli. Note also the prominent vascularity of the iris stroma. (E) The tumor infiltrate is composed of large lymphocytic cells present throughout the entire iris, (hematoxylin-eosin stain; original magnification 100×). (F) Appearance of densely packed, large cell lymphoma that overwhelms the normal loose architecture of the iris stroma (hematoxylin-eosin stain; original magnification 200×). (G) Throughout the iris there is an increased amount of vascular channels (horizontal arrows) among the normal hyalinized appearing vessels (vertical arrows) (hematoxylin-eosin stain; original magnification 400×). (H) Higher power view showing large pleomorphic tumor cells with indistinct cell borders, clumped chromatin (vertical arrow) and mitotic figures (horizontal arrow) (hematoxylin-eosin stain; original magnification 1000×). (I) Color fundus photo of the left eye months after surgery. (J) MRI brain. Axial image with FLAIR showing bilateral enhancement of the corpus callosum along with involvement of the right parietal lobe.